Hormone therapy and menopause: a protracted misunderstanding explained

Hormone replacement therapy
The most recent publications reassessing the data from trials of menopausal hormone therapy all carry the same message: hormone therapy is the most effective option for managing menopausal symptoms and when it is used in appropriate women it has minimal side effects.
- Experts, including investigators associated with the Women’s Health Initiative (WHI) clinical trial, have reached a general consensus that the original claims of harm in the WHI trial were exaggerated.
- Menopausal hormone therapy is the most effective treatment for menopausal vasomotor symptoms, and adverse events are rare in the target population (women within 10 years of their last menstrual period or before they reach 60 years of age).
- In women requiring combined oestrogen and progestogen therapy, the use of a neutral progestogen such as micronised progesterone or dydrogesterone may be associated with lower risks of breast cancer and venous thromboembolism.
- Each woman’s individual risks and needs should be assessed before initiating therapy.
- Dose and duration of therapy should be consistent with treatment goals and not governed by arbitrary time limits.
Picture credit: © Phanie/Garo/Diomedia.com
The results from the Women’s Health Initiative (WHI) clinical trial of menopausal hormone therapy (MHT) released in July 2002 cast a pall over use of MHT. Many women abruptly ceased using MHT, with inevitable consequences, and many doctors ceased prescribing MHT. Over the ensuing 14 years, debate has raged over the validity of the original WHI findings. Many publications, including several authored by WHI investigators, and data published in 2013 from long-term follow up of WHI trial participants have helped to clarify the situation.1-8 Recently, the UK National Institute for Health and Care Excellence (NICE) guideline on MHT, the International Menopause Society (IMS) recommendations on managing midlife women’s health and MHT and the global consensus statement on MHT have outlined the correct clinical management of women in midlife, including those experiencing menopausal symptoms.9-11 All carry the same message: MHT is the most effective option for managing menopausal symptoms and, when used in appropriate women, has minimal side effects.
The Women’s Health Initiative MHT trial
The WHI comprised a group of studies commissioned by the US National Institutes of Health in 1991 to address the most common causes of death, disability and impaired quality of life in postmenopausal women, that is coronary heart disease (CHD), cancer and osteoporosis.12
The WHI had three components:
- an observational study to identify predictors of disease
- a study of community approaches to developing healthy behaviour
- a clinical component comprising randomised controlled trials of three distinct interventions
- dietary modification
- calcium and vitamin D supplementation
- MHT for prevention of osteoporosis and coronary heart disease in older postmenopausal women.
Original trial protocols noted that, although much was known about the benefits and risks of MHT when given to younger peri- and postmenopausal women, much less was known about the effects of MHT initiated in women many years after their last menstrual period. The goal of the WHI randomised controlled trial of MHT was to assess health outcomes when MHT was initiated for the first time in older postmenopausal women.
The trial comprised two placebo-controlled arms. In one arm, 10,739 women who had previously undergone a hysterectomy were randomly allocated to receive conjugated equine oestrogens (CE) 0.625 mg daily or placebo.13 In the other arm, 16,608 women with an intact uterus were randomly allocated to receive placebo or CE 0.625 mg plus medroxyprogesterone acetate (MPA) 2.5 mg daily. The mean age across both arms of the study population was 63 years and the range was 50 to 79 years.14
The oestrogen and progestin arm of the trial was stopped prematurely in July 2002 because of ‘adverse outcomes’.14 At a press conference held by the Journal of the American Medical Association, journalists were told that of the women who had taken combined MHT, 29% more had a heart attack, 41% more had a stroke and 26% more developed breast cancer compared with women taking placebo. In absolute terms this amounted to seven more heart attacks, eight more strokes and eight more breast cancers per 10,000 women per year.
It was subsequently revealed that the magnitude of this harm was deliberately exaggerated by the use of relative risk estimates rather than absolute risk estimates. In comments to a journalist, the chief investigator stated that one of their goals had been to ‘shake up the medical establishment and change their thinking about hormones’.15 It later became apparent that the data had been released before complete adjudication and before review by all principal investigators and not, as had been previously planned, in age-group cohorts. Despite this, it was emphasised at the time that the results applied to all women ‘irrespective of age, ethnicity or health status’.
Data reanalysis and meta-analysis
Over the following decade there were many reanalyses of the WHI data. Many were carried out by WHI investigators and included analyses of age-group and years-since-menopause cohorts.1-4 Data from these publications pointed to a different risk–benefit profile for younger women using MHT than for older users. Despite this, the overwhelming view in both the medical and lay communities over that time remained that MHT was a dangerous intervention to be avoided wherever possible.
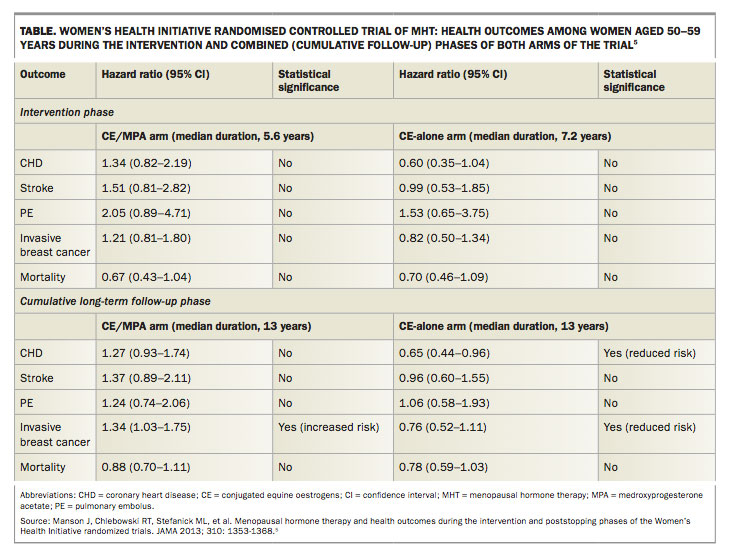
It was not until the publication of long-term follow-up data from both arms of the WHI trial that the broader medical community came to accept that many of the claims of harm reported in the original WHI paper, although perhaps true for women who were older than 70 years of age, were not true for women who were less than 60 years of age or within 10 years of their last menstrual period.5 The WHI long-term follow-up data showed that women who were 50 to 59 years of age and who used combined MHT did not have a significantly increased risk of CHD, stroke, pulmonary embolus or invasive breast cancer. Risk of venous thromboembolism (VTE) was increased as expected with oral MHT. In the oestrogen-only arm of the study long-term follow-up showed
the same small increased risk of VTE, no increased risk of stroke or pulmonary embolus and a statistically significant reduction in CHD risk. Breast cancer risk was also reduced in the oestrogen-only arm. The claim that harm occurred regardless of age was clearly wrong (Table).
{kind=link}
The original WHI claim that breast cancer increased by 26% was never made again. Moreover, subsequent reviews of the fully adjudicated data showed no increase in breast cancer risk for women in the combined MHT arm of the trial for the duration of the trial (5.6 years) unless they had used MHT prior to enrolling in the trial. Women in the oestrogen-only arm of the trial showed a nonsignificant trend towards reduced risk of breast cancer, which became a significant reduction in risk of breast cancer with long-term follow up.6
In 2015, a Cochrane systematic review commissioned to investigate the role of MHT in primary or secondary prevention of heart disease found there was no evidence to support this intervention.7 However, as with the WHI long-term follow up, they did find that women who began MHT within 10 years of their last menstrual period or before the age of 60 years had a lower risk of coronary heart disease (relative risk [RR], 0.52; 95% confidence interval [CI], 0.29–0.96), reduced all-cause mortality (RR, 0.70; 95% CI, 0.52–0.95) and no increased risk of stroke compared with placebo or no treatment. Risk of VTE was increased (RR, 1.74; 95% CI, 1.11–2.73), but this risk can be reduced or eliminated with lower-dose and nonoral therapy.8
The Cochrane review and the WHI long-term follow-up data support the view of the IMS which has, for the past decade or so, argued that the data seen in the WHI trials reflected outcomes likely to be seen in older postmenopausal women but not in those most likely to seek treatment, namely women who are in the peri- and early postmenopausal phases with troublesome vasomotor symptoms. Most women who volunteered for the WHI trial did not have any menopausal symptoms.
Effects of progestogens
Data from the WHI and other studies have shown different risk outcomes for women using an oestrogen alone compared with an oestrogen combined with some types of progestin. Either a progestin (i.e. a synthetic progestogen) or natural progesterone is required to provide endometrial protection for women with an intact uterus taking oestrogen therapy. Progesterone may have less effect on breast cancer risk than the progestin used in the WHI trial.
The largest observational study to look at the effects of different progestogens on breast cancer risk found that women who used oestrogen plus micronised progesterone had no increased risk of breast cancer (RR, 0.9; 95% CI, 0.7–1.2), whereas women using oestrogen plus other progestins had an increased risk of breast cancer (RR, 1.4; 95% CI, 1.2–1.7).16 A recent systematic review and meta-analysis of breast cancer risk with different progestogens reported a reduction in breast cancer risk for users of oestrogen plus micronised progesterone (RR, 0.67; 95% CI, 0.55–0.81).17
Studies have also shown differing cardiovascular outcomes with different progestins and progesterone when combined with oestrogen in MHT. Two large observational studies found a lower risk of VTE for users of oestrogen plus micronised progesterone compared
with oestrogen plus some synthetic progestins. In the ESTHER study, VTE risk was not increased for users of transdermal oestrogen (RR, 0.9; 95% CI, 0.4–2.1) or transdermal oestrogen plus micronised progesterone (RR, 0.7; 95% CI, 0.3–1.9) compared with nonusers, whereas risk
was increased for users of transdermal oestrogen plus progestins (RR, 3.9; 95% CI, 1.5–10.0).18 In the E3N study, which examined 549 cases of VTE over 811,643 patient-years, there was no increase in VTE risk for users of transdermal oestrogen with micronised progesterone (hazard ratio [HR], 0.9; 95% CI, 0.6–1.5), whereas the risk was increased with transdermal oestrogen plus norpregnane progestins (HR, 1.8; 95% CI, 1.2–2.7).19
The PEPI study found that the beneficial effects of oestrogen on lipoproteins were attenuated by the addition of MPA, whereas this attenuation was significantly reduced by a combination of CE and micronised progesterone.20
Perhaps the most significant effects of oestrogens on cardiovascular health are the vascular effects. A study measuring flow-mediated dilatation in nonhuman primates receiving oral CEs found a significant increase in dilatation, which
was reduced to nonsignificant change by the addition of MPA in a dose-related manner.21
Taken together, these data suggest better outcomes for women using oestrogen plus micronised progesterone compared with oestrogen plus a progestin.
Recent guidance on MHT
Over the past year several important articles have been published that improve our understanding of the true place of MHT in treating perimenopausal and postmenopausal women.
The NICE guideline on menopause management was published in November 2015.9 This very comprehensive review of the literature concluded the following:
- MHT was the most appropriate treatment for menopausal symptoms
- MHT improved bone density and reduced fracture
- in the normal target population CVD risk was not increased among women using MHT and may be reduced
- VTE risk was increased among women using oral MHT but not among women using nonoral therapy
- Breast cancer risk was not increased for women taking oestrogen but was increased with long-duration use in women taking combined oestrogen and progestin therapy. The effect reduced after ceasing therapy.
In early 2016, the IMS published new guidelines on the management of midlife women’s health and MHT.10 This comprehensive evidence-based document (freely available on the International Menopause Society website, www.imsociety.org) echoed the findings of the NICE guideline, with similar findings regarding health benefits and harms, particularly in the normal target population. Its recommendations are accompanied by levels of evidence and points to guide good practice.
An update of the global consensus statement on MHT use was also published in 2016.11 This document, much smaller and more concise than the other extremely detailed articles, summarises the place of MHT in the 21st century.
The most recent important publication is a commentary published in The New England Journal of Medicine entitled Menopause management: getting clinical ‘care back on track’.22 The authors, JoAnn Manson (WHI Principal Investigator and Steering Committee Member) and Andrew Kaunitz (WHI Principal Investigator), note that use of systemic MHT has decreased by as much as 80% among women in the USA since the release of the WHI findings. They observe that often a woman’s decision to avoid MHT is based on anxiety and confusion about the real risks of MHT. They point out that the WHI trials were designed to examine the effects of MHT in older women and are ‘now being used inappropriately in making decisions about treatment for women in their 40s and 50s who have distressing vasomotor symptoms’. In other words, there has been a misunderstanding. They further note that not only has MHT prescribing declined substantially, but a generation of new medical graduates (and younger specialists) largely lacks training and competency in managing menopausal symptoms and prescribing hormonal and nonhormonal treatments.
Manson and Kaunitz state that ‘the absolute risk of adverse outcomes is much lower in younger women than in older women; the net effect on all-cause mortality in younger women is neutral or even favourable’. They note the availability of new hormone formulations for treating postmenopausal women with vasomotor symptoms, including lower doses and transdermal routes of administration, and call for a re-evaluation of the role of MHT in the treatment of menopause. They also call for a retraining program to ensure physicians are familiar with the most appropriate treatment for postmenopausal women.
Conclusion
There is now general consensus among medical experts, including those associated with the WHI, that the original claims of harm reported in the WHI trials were exaggerated, that harm varies with the age of women and that adverse effects are extremely uncommon when MHT is prescribed to women within 10 years of their last menstrual period or before they reach 60 years of age.
Over the past decade many women have been denied safe, appropriate treatment of their menopausal symptoms because of a ‘misunderstanding’. It is time for us as clinicians to acknowledge this and to ensure that our postmenopausal patients receive the treatment they deserve; namely, effective, safe, evidence-based options. MHT is not for everyone, but for most women experiencing troublesome menopausal symptoms there is nothing better and nothing safer. MT
COMPETING INTERESTS: Professor Baber has received payment for serving on advisory boards for Pfizer and Abbott and speaking at educational meetings organised by pharmaceutical companies. He has conducted clinical research on the effects of hormonal, nonhormonal and complementary therapies on postmenopausal women. All funding of such trials has been paid into accounts administered by The University of Sydney, and Professor Baber has not benefited from such funding.
ROD BABER BPharm, MB BS, FRCOG, FRANZCOG
References
- LaCroix A, Chlebowski RT, Manson JE, et al; WHI Investigators. Health outcomes after stopping conjugated equine estrogens among postmenopausal women with prior hysterectomy: a randomized controlled trial. JAMA 2011; 305: 1305-1314.
- Chlebowski R, Hendrix SL, Langer RD, et al: WHI Investigators. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women’s Health Initiative randomized trial. JAMA 2003; 289: 3243-3253.
- Chlebowski R, Anderson GL, Gass M, et al; WHI Investigators. Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women. JAMA 2010; 304: 1684-1692.
- Anderson G, Chlebowski RT, Rossouw JE, et al. Prior hormone therapy and breast cancer risk in the Women’s Health Initiative randomized trial of estrogen plus progestin. Maturitas 2006; 55: 103-115.
- Manson J, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and poststopping phases of the Women’s Health Initiative randomized trials. JAMA 2013; 310: 1353-1368.
- Anderson GL, Chlebowski RT, Aragaki AK, et al. Conjugated equine estrogen and breast cancer incidence and mortality in postmenopausal women with hysterectomy: extended follow-up of the Women’s Health Initiative randomized placebo-controlled trial. Lancet Oncol 2012; 13: 476-486.
- Boardman H, Hartley L, Eisinga A. Hormone therapy for preventing cardiovascular disease in post-menopausal women. Cochrane Database Syst Rev 2015; (3): CD 002229.
- Scarabin PY. Hormone therapy and venous thromboembolism among postmenopausal women. Front Horm Res 2014; 43: 21-32.
- National Institute for Health and Care Excellence. Menopause: diagnosis and management (NICE guideline). November 2015. Available online at:
- http://www.nice.org.uk/guidance/ng23 (accessed January 2017).
- Baber R, Panay N, Fenton A; International Menopause Society (IMS) Writing Group. 2016 IMS recommendations on women’s midlife health and menopause hormone therapy. Climacteric 2016; 19: 109-150.
- de Villiers T, Hall JE, Pinkerton JV, et al. Revised global consensus statement on menopausal hormone therapy. Climacteric 2016; 19: 313-315.
- The Women's Health Initiative Study Group. Design of the Women’s
- Health Initiative clinical trial and observational study. Control Clin Trials 1998; 19: 61-109.
- Anderson GL, Limacher M, Assaf AR; Women’s Health Initiative Steering Committee. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy. the Women's Health Initiative Randomized Controlled Trial. JAMA 2004: 291; 1701-1712.
- Rossouw J, Anderson GL, Prentice RL, et al; Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA 2002; 288: 321-333.
- Parker-Pope T. The hormone decision. Emmaus, PA: Rodale Books; 2007.
- Fournier A, Berrino F, Riboli E, Avenel V, Clavel-Chapelon F. Breast cancer risk in relation to different types of hormone replacement therapy in the E3N-EPIC cohort. Int J Cancer 2005; 114: 448-454.
- Asi N, Mohammed K, Haydour Q, et al. Progesterone vs. synthetic progestins and the risk of breast cancer: a systematic review and meta-analysis. Syst Rev 2016; 5: 121.
- Canonico M et al. Hormone therapy and venous thromboembolism among postmenopausal women: impact of the route of estrogen administration and progestogens: the ESTHER Study. Circulation 2007; 115: 840-845.
- Canonico M, Fournier A, Carcaillon L, et al. Postmenopausal hormone therapy and risk of idiopathic venous thrombosis. Results from the E3N cohort study. Arterioscler Thromb Vasc Biol 2010; 30: 340-345.
- Judd HL, Mebane-Sinis I, Legault C, et al. Effects of hormone replacement therapy on endometrial histology in post menopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) trial. JAMA 1996; 275: 370-375.
- Register T, Adams MR, Golden DL, Clarkson TB. Conjugated equine estrogens alone, but not in combination with medroxyprogesterone acetate, inhibit aortic connective tissue remodeling after plasma lipid lowering in female monkeys. Arterioscler Thromb Vasc Biol 1998; 18: 1164-1171.
- Manson JE, Kaunitz AM. Menopause management – getting clinical care back on track. N Engl J Med 2016; 374: 803-806.