Appropriate nutrition and diet after MI

Diet
Myocardial infarction
Many people who have had a myocardial infarction continue to consume a low-quality diet. Educating patients on the principles behind evidence-based high-quality diets rather than providing prescriptive dietary plans will equip them to minimise their future risk.
- Cardiovascular disease is the leading cause of death worldwide.
- Modest weight reduction in individuals after myocardial infarction (MI) reduces all-cause mortality and subsequent acute cardiovascular events.
- High-quality diets reduce all-cause and cardiovascular mortality after MI.
- Health practitioners should focus on educating patients who have had an MI on the principles behind weight reduction and evidence-based quality diets such as the Alternative Healthy Eating Index 2010 or the Mediterranean diet, rather than prescriptive dietary plans.
Picture credit: © udra11/stock.adobe.com
Cardiovascular disease is currently the leading cause of death worldwide. Globally, 17.7 million people died from cardiovascular disease in 2016. Of these deaths, 7.4 million were due to ischaemic heart disease.1 Five-year mortality remains high among patients treated between 1989 and 1993, at around 21%.2
Maintaining a healthy body mass index after a myocardial infarction (MI) is recommended by the American College of Cardiology and American Heart Association (ACC/AHA).3 However, the long-term effects of a diet aimed at weight loss and the potential effects of malnutrition after MI are unknown. Areas of burgeoning interest include the effects different diets may have on mortality and morbidity among patients who have had an MI and the potential role of omega-3 fatty acid supplementation.
In this article, we review the latest evidence concerning diet and nutrition after MI, with a focus on the Mediterranean diet and omega-3 fatty acid supplementation. Finally, we will highlight the importance of the role of nutrition, diet and weight loss in the context of an increasing prevalence of obesity, type 2 diabetes and the metabolic syndrome in the general population, and therefore in the population who have survived MI.4
Diet after myocardial infarction
Changes in the lifestyle of people who have survived an MI, including improvements in diet, have been shown to reduce all-cause mortality by 20 to 35%.5-7 Despite patients being educated on the potential benefits of dietary changes, only 43.4% of patients with coronary heart disease in high-income countries and 25.8% in low-income countries were considered to have a healthy post-MI dietary pattern.8
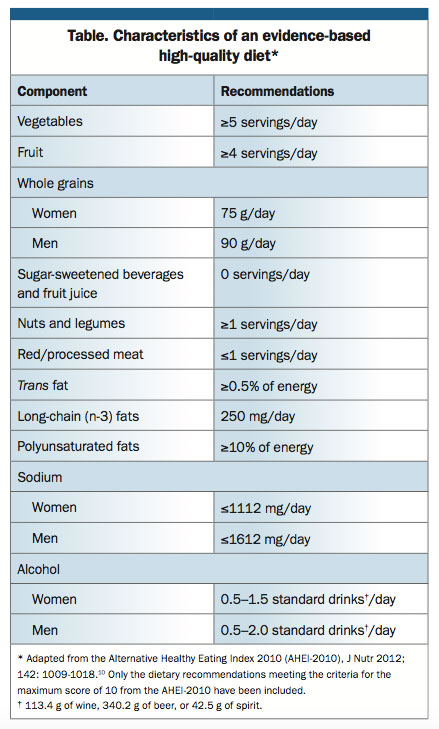
A recent prospective study among survivors of MI investigated the association between all-cause and cardiovascular mortality and both diet quality after MI and the changes to diet before and after MI.9 The prospective cohort included 2258 women registered in the Nurses’ Health Study and 1840 men registered in the Health Professionals Follow-up Study. Participants were free of cardiovascular disease, stroke or cancer and had survived a first MI during follow up. The median survival time after an initial MI was 8.7 years for women and 9.0 years for men. There were 682 deaths from all causes and 336 deaths from a cardiovascular cause among the women, and 451 and 222, respectively, among the men. Diet quality was measured using the Alternative Healthy Eating Index 2010 (AHEI 2010; Table), which is based on foods and nutrients that are predictive of chronic disease risk.10
{kind=link}
A high score on the AHEI 2010 after MI, indicative of meeting the criteria for an evidence-based high-quality diet, was associated with a 24% lower mortality from all causes and 26% lower mortality from cardiovascular disease, comparing extreme quintiles. Greater improvement of diet quality from before to after MI was associated with 30% lower mortality from all causes and 40% lower mortality from cardiovascular disease. The greatest changes made by MI patients were reducing saturated and trans fat intakes.9 Relative risk for chronic disease, particularly for coronary heart disease and diabetes, was significantly lower for individuals meeting the AHE1 2010 high-quality diet criteria compared with those who did not (p<0.001).10 The results of this study highlight the ongoing need for health practitioners to continue reinforcing the importance of dietary choices to patients who have had an MI.
The optimal dietary pattern for survivors of MI is not well understood. The 2013 ACC/AHA guidelines recommend a diet that emphasises intake of vegetables, fruits and whole grains for patients who would benefit from LDL-cholesterol and blood-pressure lowering. This should include low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils and nuts and limited intake of sweets, sugar-sweetened beverages and red meats. For patients who would benefit from LDL-cholesterol lowering, calories from saturated fat should be limited to 5 to 6% of total calories, and calories from trans-fat should be reduced. Specific recommendations for patients who would benefit from lowering blood pressure include reducing sodium intake to no more than 2400 mg per day.11 The 2012 European Society of Cardiology guidelines on cardiovascular disease prevention (both primary and secondary) make a strong recommendation for a healthy diet, defined as having the following characteristics: less than 10% of total energy intake as saturated fatty acids; as little as possible of trans-unsaturated fatty acids; 30 to 45 g of fibre per day; 200 g of fruit per day; 200 g of vegetables per day; and fish at least twice a week, one serving of which should be oily fish.12 Of note, most of these dietary recommendations are based on similar principles and dietary caloric distribution to both the AHEI-2010 and the Mediterranean diet.
The Mediterranean diet
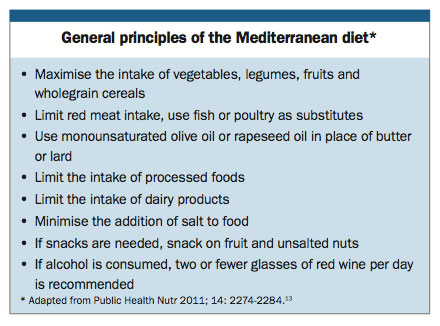
Like the AHEI-2010, the Mediterranean diet does not single out specific food items, but rather emphasises an abundance of plant foods and fresh fruit along with moderate amounts of wine and low amounts of red meat and salt (Box).13 In addition, the Mediterranean diet recommends olive oil as the principal source of fat, limited dairy intake and consumption of moderate amounts of fish and poultry. Findings from several randomised controlled trials have suggested that following the Mediterranean diet potentially reduces the risk of repeat cardiovascular events.14,15
{kind=link}
The Lyon Diet Heart Study among people who had had a first MI was one of the first randomised dietary secondary-prevention studies to report mortality benefits associated with a Mediterranean diet.14 Over a mean follow-up period of 46 months, a reduction in cardiac death and nonfatal MI was shown among participants who consumed a Mediterranean-type diet (14 events vs 44 in the prudent Western-type diet group; p=0.0001). The Mediterranean type diet was supplemented by a margarine with saturated fatty acid and oleic acid content comparable to olive oil, and a higher content of alpha-linolenic acid (a key constituent of walnuts). The protective effect of the Mediterranean dietary pattern was maintained up to four years after a first MI.
In a multicentre randomised controlled trial published in 2013, among people at high cardiovascular risk, a Mediterranean diet supplemented with extra-virgin olive oil or nuts reduced the incidence of major cardiovascular events.16 In this trial, 7447 individuals with high cardiovascular risk were assigned to one of three diets: a Mediterranean diet supplemented with extra-virgin olive oil (four or more tablespoons per day); a Mediterranean diet supplemented with mixed nuts (three or more serves per week, with a 30 g serve composed of 15 g walnuts, 7.5 g almonds, and 7.5 g hazelnuts); or a control diet comprising advice to reduce dietary fat. The primary endpoint was the rate of major cardiovascular events (myocardial infarction, stroke, death from cardiovascular causes). A primary endpoint event occurred in 288 participants. There were 109 events among the control group, 96 events among the group assigned to a Mediterranean diet with extra-virgin olive oil (hazard ratio [HR], 0.70; 95% CI, 0.54–0.92) and 83 events in the group assigned to a Mediterranean diet with nuts (HR, 0.72; 95% CI, 0.54–0.96). On the basis of the interim results and the foreseen benefits of the Mediterranean diet, the trial was stopped after a median follow up of 4.8 years.
Despite the growing evidence for an inverse association between adherence to the Mediterranean diet and cardiovascular risk, it is important to acknowledge that dietary interventions used in studies may be difficult to replicate and comply with outside of a research setting. For example, consuming a minimum of four tablespoons of olive oil per day is equivalent to almost half a litre per week, which may be a significant volume for many people. Further, the components and quantities making up the Mediterranean diet for each study differed, making it difficult to formulate a single diet from the many evidence-based dietary interventions. However, given the growing evidence and potential benefits surrounding adherence to the Mediterranean diet after an MI, patients should receive education on the general principles of the Mediterranean diet.
Omega-3 fatty acid supplementation
Early trials evaluating the effect of omega-3 fatty acids have reported benefits for mortality and cardiovascular events.17,18 On the basis of the positive results of these early trials, various clinical guidelines recommend the use of omega-3 fatty acid supplements to reduce mortality and cardiovascular risk.19 However, recent larger trials have reported no benefit of omega-3 fatty acids on cardiovascular outcomes.19
A recent systematic review and meta-analysis reviewed 20 randomised controlled trials including 62,851 participants.19 Mean follow-up periods ranged from six months to six years. Daily doses of eicosapentaenoic acid and docosahexaenoic acid ranged between 464 to 1860 mg and 335 to 1500 mg, respectively, compared with recommended dietary intakes of 250 to 2000 mg per day for each. Composition of placebos included corn oil and olive oil. There were no significant differences between groups for the primary composite cardiovascular outcome or for total and nonvascular mortality, coronary events, revascularisation and arrhythmias. Vascular death was the only outcome for which a significant benefit was detected (relative risk [RR], 0.86; 95% CI, 0.75–0.99; p=0.03). It may be argued that trials including patients already on optimal therapy to protect against cardiovascular risk, such as antihypertensive medications, statins and antiplatelet agents, may dilute the detectable effect of taking an omega-3 fatty acid supplement.
Adverse events were more common among trial participants taking omega-3 fatty acid supplements compared with those taking a placebo (RR, 1.18; 95% CI, 1.02-1.37; p=0.03). Side effects of omega-3 fatty acid supplements include nausea, diarrhoea, other mild gastrointestinal disturbances and a theoretical increased risk of bleeding.19,20
Given these findings, it appears reasonable for patients with existing vascular disease who are currently using omega-3 fatty acid supplements to continue to do so, but stronger evidence is required to support widespread use, particularly among lower-risk patients.
Caffeine after acute MI
Until recently, it has remained unclear whether caffeine is cardioprotective in individuals who have already experienced an MI. Observational studies have suggested that consuming small or moderate amounts of coffee (six or fewer cups/day) has no adverse impact on cardiovascular disease risk.21-23 However, one small case–control study with 117 cases suggested that heavy coffee consumption (more than ten cups/day) may be associated with an increased risk of sudden cardiac arrest in patients with pre-existing coronary artery disease.24
A recent meta-analysis of prospective studies examined the relationship between coffee intake and mortality after MI.25 Two eligible studies identified a total of 3271 participants with a mean follow-up duration of 3.8 years. Light coffee consumption was defined as one to two cups per day and heavy consumption as more than two cups per day. One paper specified a cup volume of 150 ml, whereas the cup volume was not quantified in the other study. Coffee preparation and the maximum number of cups per day were not recorded. Light coffee drinkers were shown to have reduced all-cause mortality compared with those who did not drink coffee (HR, 0.79; 95% CI, 0.66–0.94; p=0.008). The inverse correlation was more marked among heavy coffee drinkers compared with noncoffee drinkers (HR, 0.54; 95% CI, 0.45–0.65; p<0.00001). Heavy (>2 cups/day) versus light (1–2 cups/day) coffee drinking was also associated with a reduced mortality risk (HR, 0.69; 95% CI, 0.58–0.83; p<0.0001). However, in one study among individuals who drank more than seven cups per day, the mortality benefit was lost (HR, 1.14; 95% CI, 0.81–1.60). Given that these results appear to show no deleterious cardiovascular outcomes and that caffeine may have potential mortality benefits at small to moderate amounts, patients who have had an MI can be advised that they may continue to consume caffeine, while being mindful that these data are limited to two studies and that excessive coffee consumption may be associated with sudden cardiac arrest.
The changing population and the role of secondary prevention
The prevalence of obesity has doubled worldwide between 1980 and 2008. Globally, 44% of diabetes and 23% of ischaemic heart disease are attributable to being overweight or obese.26,27
In 2012, the AHA analysed changes in clinical and demographic characteristics of patients at increased risk for cardiovascular events.4 The retrospective study included data from 138,122 patients requiring admission for an acute MI between 2003 and 2008. At least one of five modifiable classic risk factors (hypertension, hyperlipidaemia, current smoking, diabetes mellitus and obesity) was reported by 93% of patients, and 69% reported two or more. From 2003 to 2008 among the 45,172 patients who had had ST-segment elevation MI, there was an increased prevalence of:
- obesity, increased from 29.7 to 30.82% (p<0.0001)
- low HDL cholesterol levels (<1.0 mmol/L in men, <1.3 mmol/L in women), increased significantly from 42.86 to 52.32% (p<0.0001)
- high LDL cholesterol levels (>2.6 mmol/L), increased from 37.2 to 39.95% (p<0.0001)
- high triglyceride levels (>1.7 mmol/L), increased from 26.27 to 27.02% (p=0.0004).
The authors suggest that continued increases in the prevalences of metabolic syndrome components such as obesity and low HDL cholesterol over the next decade, along with persisting high prevalences of hypertension and diabetes, may offset the beneficial clinical effects of decreasing trends in other risk factors and could result in higher disease burden and post-MI morbidity in MI survivors.
The reversible risk factors comprising the metabolic syndrome, including elevated waist circumference, elevated triglycerides, reduced HDL cholesterol, hypertension and elevated fasting glucose, need to be addressed among MI survivors.28 The mainstays of treatment are lifestyle interventions to improve central obesity and insulin resistance.29 The NHMRC obesity management guidelines recommend weight loss interventions based on caloric restriction (including reducing portion size and consumption of high energy foods), increased physical activity and behaviour modification, with the goal of achieving a 5 to 10% reduction in weight.30
In a study of 377 consecutive patients (mean age of 62 ± 11 years) enrolled in a cardiac rehabilitation program and followed for a mean of 6.4 years, weight loss was a marker of a more favourable long-term cardiovascular outcome in patients post MI. Patients who lost weight lost on average 3.6 ± 4.1 kg, whereas those who did not lose weight gained on average 1.5 ± 1.4 kg. The rate of the composite outcome (total mortality and acute cardiovascular events) was 24% in those who did lose weight compared with 37% in those who did not lose weight (p<0.001). The difference remained significant after adjusting for obesity status, and participants with a baseline body mass index of 25 kg/m2 or more benefited similarly to those with a body mass index of less than 25 kg/m2.31 A focus on weight loss and reducing metabolic risk factors through quality diet and exercise for patients who have had an MI may therefore be more important than strict dietary regimes.
Conclusion
There is substantial evidence for the benefits of even modest weight reduction in cardiovascular disease, particularly among patients who have had an MI, in whom overweight and obesity are common; yet the role of dietary patterns and supplementation in cardiovascular disease requires further research.
Cardiovascular risk factor management and weight loss through the combination of exercise and evidence-based high-quality diets should be emphasised for patients who have had an MI. It is well recognised that a healthy dietary pattern reduces all-cause and cardiovascular mortality after MI; however, a large number of people who have had an MI continue to have low-quality diets. These patients should be given dietary advice, but the focus should be on educating them in the principles behind evidence-based quality diets such as the AHEI-2010 or the Mediterranean diet, rather than prescriptive dietary plans.
Low to moderate caffeine consumption appears to be safe for patients who have had an MI. Given the conflicting findings with regard to omega-3 fatty acid supplementation and the potentially increased risk of gastrointestinal side-effects with supplementation, it would be reasonable for patients with existing vascular disease who are currently taking omega-3 fatty acids to continue to do so, but stronger evidence is required to support starting therapy among lower risk patients.
References
- World Health Organization. The top 10 causes of death 2016. Available online at: http://www.who.int/mediacentre/factsheets/fs310/en (accessed June 2017).
- Bata IR, Gregor RD, Wolf HK, Brownell B. Trends in five-year survival of patients discharged after acute myocardial infarction. Can J Cardiol 2006; 22: 399-404.
- Anderson JL, Adams CD, Antman EM, et al; American College of Cardiology; American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction); American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons; American Association of Cardiovascular and Pulmonary Rehabilitation; Society for Academic Emergency Medicine. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol 2007; 50: e1-e157.
- Boyer NM, Laskey WK, Cox M, et al. Trends in clinical, demographic, and biochemical characteristics of patients with acute myocardial infarction from 2003 to 2008: a report from the American Heart Association get with the guidelines coronary artery disease program. J Am Heart Assoc 2012; 1: e001206.
- Weiner SD, Rabbani LE. Secondary prevention strategies for coronary heart disease. J Thromb Thrombolysis 2010; 29: 8-24.
- Scrutinio D. The potential of lifestyle changes for improving the clinical outcome of patients with coronary heart disease: mechanisms of benefit and clinical results. Rev Recent Clin Trials 2010; 5: 1-13.
- Iestra JA, Kromhout D, van der Schouw YT, Grobbee DE, Boshuizen HC, van Staveren WA. Effect size estimates of lifestyle and dietary changes on all-cause mortality in coronary artery disease patients: a systematic review. Circulation 2005; 112: 924-934.
- Teo K, Chow CK, Vaz M, Rangarajan S, Yusuf S; PURE Investigators Writing Group. The Prospective Urban Rural Epidemiology (PURE) study: examining the impact of societal influences on chronic noncommunicable diseases in low-, middle-, and high-income countries. Am Heart J 2009; 158: 1-7.e1.
- Li S, Chiuve SE, Flint A, et al. Better diet quality and decreased mortality among myocardial infarction survivors. JAMA Intern Med 2013; 173: 1808-1818.
- Chiuve SE, Fung TT, Rimm EB, et al. Alternative dietary indices both strongly predict risk of chronic disease. J Nutr 2012; 142: 1009-1018.
- Eckel RH, Jakicic JM, Ard JD, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; 63(25 Pt B): 2960-2984.
- Perk J, De Backer G, Gohlke H, et al; European Association for Cardiovascular Prevention and Rehabilitation (EACPR); ESC Committee for Practice Guidelines (CPG). European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Eur Heart J 2012; 33: 1635-1701.
- Bach-Faig A, Berry EM, Lairon D, et al; Mediterranean Diet Foundation Expert Group. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr 2011; 14: 2274-2284.
- de Lorgeril M, Salen P, Martin JL, Monjaud I, Delaye J, Mamelle N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of the Lyon Diet Heart Study. Circulation 1999; 99: 779-785.
- de Lorgeril M, Renaud S, Mamelle N, et al. Mediterranean alpha-linolenic acid-rich diet in secondary prevention of coronary heart disease. Lancet 1994; 343: 1454-1459.
- Estruch R, Ros E, Salas-Salvado J, et al; PREDIMED Study Investigators. Primary prevention of cardiovascular disease with a Mediterranean diet. N Engl J Med 2013; 368: 1279-1290.
- Siscovick DS, Raghunathan TE, King I, et al. Dietary intake and cell membrane levels of long-chain n-3 polyunsaturated fatty acids and the risk of primary cardiac arrest. JAMA 1995; 274: 1363-1367.
- Albert CM, Campos H, Stampfer MJ, et al. Blood levels of long-chain n-3 fatty acids and the risk of sudden death. N Engl J Med 2002; 346: 1113-1118.
- Kotwal S, Jun M, Sullivan D, Perkovic V, Neal B. Omega 3 fatty acids and cardiovascular outcomes: systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes 2012; 5: 808-818.
- Australian Government Department of Health TGA. Medicines Safety Update No.2; 2010. Safety of fish oil and omega-3 fatty acids 2010. Canberra: Department of Health; 2010. Available online at: https://www.tga.gov.au/publication-issue/medicines-safety-update-no2-2010 (accessed June 2017).
- Lopez-Garcia E, van Dam RM, Willett WC, et al. Coffee consumption and coronary heart disease in men and women: a prospective cohort study. Circulation 2006; 113: 2045-2053.
- Grobbee DE, Rimm EB, Giovannucci E, Colditz G, Stampfer M, Willett W. Coffee, caffeine, and cardiovascular disease in men. N Engl J Med 1990; 323: 1026-1032.
- Kleemola P, Jousilahti P, Pietinen P, Vartiainen E, Tuomilehto J. Coffee consumption and the risk of coronary heart disease and death. Arch Intern Med 2000; 160: 3393-3400.
- de Vreede-Swagemakers JJ, Gorgels AP, Weijenberg MP, et al. Risk indicators for out-of-hospital cardiac arrest in patients with coronary artery disease. J Clin Epidemiol 1999; 52: 601-607.
- Brown OI, Allgar V, Wong KY. Coffee reduces the risk of death after acute myocardial infarction: a meta-analysis. Coron Artery Dis 2016; 27: 566-572.
- World Health Organization. Obesity and overweight: fact sheet (updated June 2016). Available online at: http://www.who.int/mediacentre/factsheets/fs311/en (accessed June 2017).
- World Health Organization. Fact file: ten facts on obesity. Fact 4. Available online at: http://www.who.int/features/factfiles/obesity/facts/en/index3.html (accessed June 2017).
- Harris MF. The metabolic syndrome. Aust Fam Physician 2013; 42: 524-527.
- de Lorgeril M. Commentary on the clinical management of metabolic syndrome: why a healthy lifestyle is important. BMC Med 2012; 10: 139.
- National Health and Medical Research Council. Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia (2013). Melbourne: National Health and Medical Research Council; 2013. Available online at: www.nhmrc.gov.au/guidelines/publications/n57 (accessed June 2017).
- Sierra-Johnson J, Romero-Corral A, Somers VK, et al. Prognostic importance of weight loss in patients with coronary heart disease regardless of initial body mass index. Eur J Cardiovasc Prev Rehabil 2008; 15: 336-340.