What to do about missing IUD threads

Women's health
During routine cervical screening, the threads of a patient’s copper IUD are not visible. What is the best approach to manage this common clinical presentation?
Case scenario
Sara, aged 32 years, presents for routine cervical screening. She had a copper intrauterine device (IUD) inserted two years ago and on examination you are unable to see the threads at the cervical os. She says she has never attempted to check the threads herself and is unaware of the IUD being expelled.
Commentary
There are several possible reasons for the discovery of missing IUD threads.
- The IUD is in the correct intrauterine position but the threads have retracted into the cervical canal or uterine cavity.
- The IUD has been expelled without the patient noticing.
- Uterine perforation has occurred, either partially into the myometrium or completely into the peritoneal cavity.
- The IUD has failed and the threads have been pulled up into the uterine cavity with pregnancy.
Although retraction of the threads into the cervical canal or uterine cavity is likely to be the most common cause of missing IUD threads, data are lacking about how frequently this occurs.
Expulsion of the IUD is estimated to occur in about 5% of women, mostly in the first few months after insertion (expulsion of a copper IUD may go unnoticed within the context of a heavy menstrual period).1 The risk of perforation is about one per 500 insertions, with higher rates among postnatal and breastfeeding women.2 Women with either expulsion of the IUD or uterine perforation may be asymptomatic.
Device failure resulting in pregnancy occurs in fewer than one in 100 women, and is usually detected within the first 12 weeks of gestation when the IUD threads may still be visible within the vagina.3
Urgent consideration of an ectopic pregnancy is essential in all women with an IUD inserted and a positive pregnancy test regardless of whether IUD threads are visible or not. A higher percentage of pregnancies that occur with an IUD in situ are ectopic; however, the absolute incidence of ectopic pregnancies in women using a copper IUD is very low at 0.08 per 100 women years.4
Important details of the patient history
When taking a patient history, it is important to enquire about any changes to the menstrual bleeding pattern including lighter periods (which could indicate expulsion) or missed periods (suggestive of pregnancy), or any abnormal vaginal bleeding, pelvic pain or vaginal discharge (which could be associated with perforation). You should also enquire about the timing of the patient’s last normal menstrual period and last sexual intercourse.
Next steps
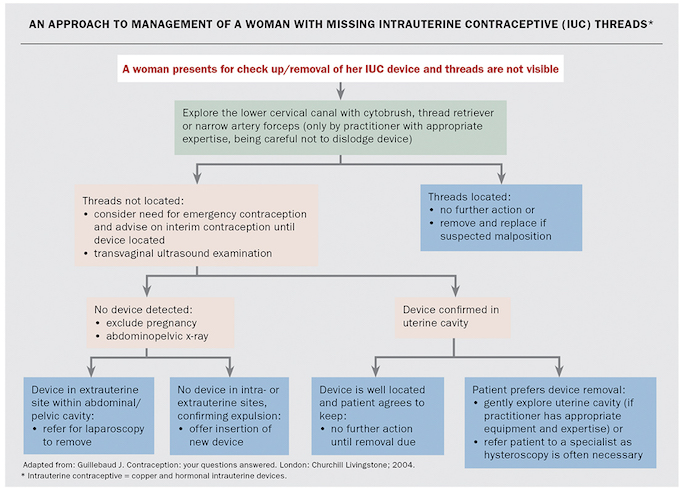
Visual inspection of the cervix with a good light source is important to check for retracted threads or threads that have been cut very short within the canal (Flowchart). A sterile swab or cytobrush can be useful to assess whether the threads are just within the external cervical os. A bimanual pelvic examination is required if the woman has symptoms of pain, discharge or abnormal bleeding.
{kind=link}
Sara has not noticed any change to her periods and has no pain or other symptoms. She has not had sexual intercourse in the past month because her partner has been overseas but he is coming home tomorrow.
Pregnancy considerations
It is essential to perform a urine pregnancy test for all sexually active women with missing IUD threads. It is worth remembering that a very early pregnancy may be associated with a false-negative result if unprotected intercourse has occurred within the previous three weeks. A positive pregnancy test in the context of missing IUD threads is most likely to be associated with an expelled device, but pregnancy can also occur with an IUD in the uterus or when the device has perforated the uterus.
Sara’s pregnancy test is negative and she is advised to use alternative contraception or abstain from sexual intercourse until the IUD is located. Sara says she will use condoms until the IUD is located.
If intercourse had occurred within the past few days an emergency contraceptive pill could have been offered. The 1.5 mg levonorgestrel emergency contraceptive pill is licensed for up to 72 hours after unprotected intercourse but has proven effectiveness up to four days, whereas ulipristal acetate is licensed for up to five days after unprotected sex.
Determining the location of the IUD
The first-line radiological investigation for missing IUD threads is a transvaginal ultrasound (TVUS) examination. If the IUD is not found to be located within the uterus on ultrasound examination then it cannot be assumed that it has been expelled. A plain abdominopelvic x-ray is needed to check for a perforated device in the pelvis or abdomen.
It is useful to give additional instructions on the referral
form (‘TVUS +/- plain abdominopelvic x-ray if the IUD is not seen within the uterine cavity and pregnancy is excluded’). This will avoid the need for a repeat radiology visit.
Subsequent management based on outcomes of investigations
IUD located within the uterus
Most clinicians would not advise any intervention if an IUD with missing threads appears well positioned within the uterus on ultrasound imaging. However, the possibility of undetected future expulsion must be discussed because the patient now cannot check the threads herself regularly. The potential risks and costs of removal and re-insertion of the IUD usually outweigh the small risk of undetected future expulsion but some women may choose this course of action.
IUD located outside the uterus
If the IUD is found to have either partially or completely perforated through the myometrium into the peritoneal cavity, the patient should be referred to a specialist for laparoscopic removal.
Pregnancy with an IUD in situ
It is essential to consider the possibility of an ectopic pregnancy at the time of the positive pregnancy test, and to refer the patient promptly for a pelvic ultrasound examination. Any woman with symptoms or signs of an ectopic pregnancy should be referred urgently to a hospital emergency department.
A positive result on a pregnancy test for a woman with missing IUD threads is likely to be a surprise – sensitive discussion of pregnancy options is required. For women wishing to continue the pregnancy, removal of the device as soon as possible under ultrasound guidance is advised before 12 weeks’ gestation. It should be explained to the patient that although removal may be associated with a small increased risk of miscarriage, retention of the IUD greatly increases the risks of pregnancy-related complications including infection, miscarriage and premature delivery.
If termination of pregnancy is requested then the IUD could be removed at the same time as a surgical abortion. Medical termination of pregnancy is contraindicated for women with an IUD in situ that cannot be removed.
Outcome
On TVUS examination, Sara’s IUD is found to be appropriately located 1 cm from the uterine fundus and she is happy to keep using it until its expiry.
Conclusion
Checking for IUD threads is part of all post-insertion checks and should be performed opportunistically whenever a speculum examination is performed.
Key points in the management of patients with missing IUD threads include:
- always perform a urine pregnancy test and exclude an ectopic pregnancy if the test is positive
- never assume expulsion of the IUD if the uterus is empty on TVUS examination; order an abdominopelvic x-ray to check for perforation
- recommend alternative contraception until the device is located.
Competing interests: Dr Bateson and Dr South have attended expert advisory forums run by Bayer Healthcare. Dr Bateson has also received support to attend conferences from Bayer Healthcare. Family Planning NSW receives sponsorship for educational courses from Bayer Healthcare and Medical Industries.
References
- A randomized multicentre trial of the Multiload 375 and TCu380A IUDs in parous women: three-year results. UNDP/UNFPA/WHO/World Bank, Special Programme of Research, Development and Research Training in Human Reproduction: IUD Research Group. Contraception 1994; 49: 543-549.
- Heinemann K, Reed S, Moehner S, Do Minh T. Risk of uterine perforation with levonorgestrel-releasing and copper intrauterine devices in the European Active Surveillance Study on Intrauterine Devices. Contraception 2015; 91: 274-279.
- Trussell J. Contraceptive failure in the United States. Contraception 2011; 83: 397-404.
- Heinemann K, Reed S, Moehner S, Do Minh T. Comparative contraceptive effectiveness of levonorgestrel-releasing and copper intrauterine devices: the European Active Surveillance Study on Intrauterine Devices. Contraception 2015; 91: 280-283.