Peer Reviewed
ECG education
Chemotherapy-induced cardiomyopathy
Recent articles on:
Cancer chemotherapy
Cancer chemotherapy
Abstract
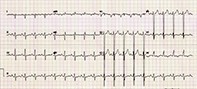
A 61-year-old woman presents with new persistent ankle swelling and mild shortness of breath two years after receiving chemotherapy for breast cancer. What does her ECG show?
Key Points
- Chemotherapy-induced cardiotoxicity may be severe and develop into cardiomyopathy (type I) or may be transient (type II).
- Common ECG abnormalities due to chemotherapy-induced cardiomyopathy include nonspecific ST wave changes and T wave flattening and a decreased QRS voltage. Other more significant abnormalities may include left ventricular hypertrophy (S wave in lead V2 >35 mm) and right axis deviation indicating biventricular enlargement; left atrial enlargement (deep, wide negative P wave in lead V1); and right atrial enlargement (peaked P wave in lead II).
- The ECG is also useful to exclude other possible causes of cardiac symptoms, such as ischaemia, conduction abnormalities and atrial arrhythmias.
- Risk factors for type I chemotherapy- induced cardiotoxicity include cumulative dose and rate of chemotherapy (especially when the anthracycline doxorubicin is used), female sex, use of mediastinal radiotherapy, either advanced age or younger age, and the presence of pre-existing hypertension or pre-existing heart disease.
Purchase the PDF version of this article
Already a subscriber? Login here.