Pregnancy and rheumatoid arthritis: it’s not all doom and gloom

Health problems in pregnancy
Rheumatoid arthritis
Contrary to common belief, some medications to treat rheumatoid arthritis (RA) are safe to use during the preconception period, pregnancy and breastfeeding. As uncontrolled RA is associated with subfertility and poor outcomes for both mother and baby, management should be individualised, balancing risks of active disease against any medication-related risks.
Pregnancy is relatively common in women with rheumatoid arthritis (RA) and poses unique management challenges. The reported prevalence of RA is 1 to 2 per 1000 women, which translates to an estimated 5000 to 10,000 Australian women of childbearing age with RA.1,2 The average birth rate in Australia of 65 per 1000 women gives an estimate of up to 1300 pregnancies in women with RA per year in Australia.
Many of these women will have been treated with disease-modifying antirheumatic drugs (DMARDs) to minimise pain and joint damage. Some will have stopped all medications before or shortly after conception, fearful of the adverse effects on the fetus, willing to ignore their pain and suffering for the ‘benefit’ of their baby. Many will remain anxious about the safety of medications, including DMARDs, for their babies. Almost all will be unaware of the adverse effects of uncontrolled RA on their pregnancy.
This article discusses the management of women with RA before, during and after pregnancy, including choice of appropriate medications to treat this potentially devastating disease.
Relation between RA, fertility and pregnancy
RA and fertility
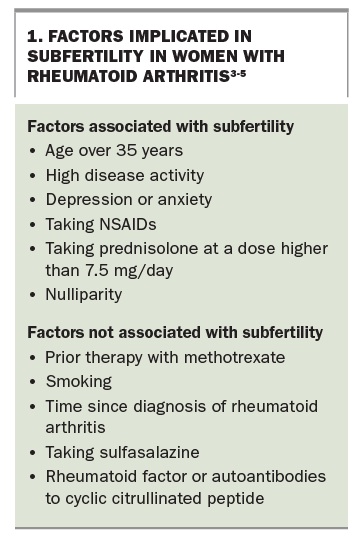
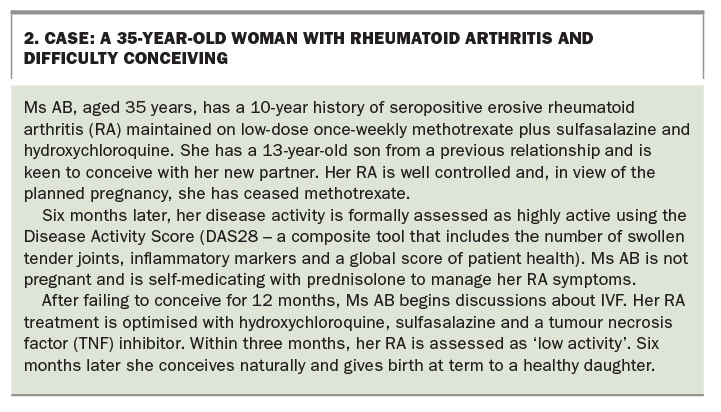
Women with RA have smaller-sized families on average. The reasons for this may include delay in pursuing pregnancy or an inability to conceive caused by poor disease control, suboptimal medication use, and other patient, physician and psychosocial factors. Nearly one-third of patients with RA required longer than 12 months to conceive, and 15% were unable to conceive.3 Factors implicated in subfertility in women with RA are shown in Box 1.3-5 A case that illustrates the potential effects of RA on fertility is described in Box 2.
{kind=link}
{kind=link}
Impact of pregnancy, birth and breastfeeding on RA
In the past it has been reported that RA improves during pregnancy in all patients. Indeed, early small retrospective studies suggested that it did improve in 75 to 90% of women with RA. However, since substantial advances in the management of patients with RA, population-based studies have shown that only about 25% of women remain in remission throughout pregnancy.6,7
Postnatal RA flares are common. A 1999 study showed that 80 to 90% of patients with RA had a flare within three months of giving birth.6 However, a study a decade later reported that only 39% had a flare by 26 weeks after the birth. The difference in postpartum flare rates may be explained by continued or early recommencement of DMARDs in the later cohort.7
As postnatal flares are common, it is difficult to know whether breastfeeding further increases the risk. There are numerous benefits of breastfeeding for both women and their babies. Women with RA who want to breastfeed should be encouraged to do so but supported if they choose not to.
RA and pregnancy outcome
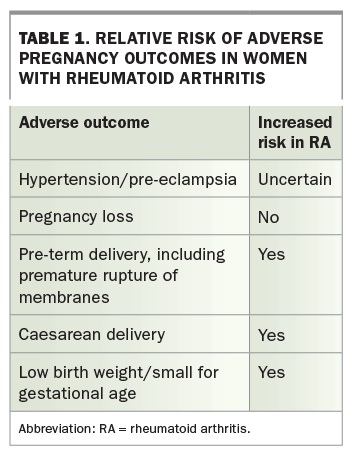
The relative risk of adverse pregnancy outcomes in women with RA is shown in Table 1. To date, published data are unclear as to whether patients with RA who are pregnant have higher rates of maternal hypertension and pre-eclampsia.8,9 Pregnancy loss does not seem to be increased among patients with RA. Preterm birth, Caesarean delivery and low-birth-weight and small-for-gestational-age infants are more common among women with RA.9 Preterm birth is most common among patients with moderate-to-severe disease activity.10
{kind=link}
As the long-term adverse outcomes of small-for-gestational-age infants include an increased risk of cardiovascular mortality, hypertension and diabetes in adulthood, the potential impact of uncontrolled RA activity on both maternal and fetal outcomes should be taken into account.11
RA medication and pregnancy
In assessing the overall impact of RA medication on the fetus, the following should be taken into account:
- the specific medication
- gestational age
- the risk to the mother and fetus if RA is untreated.
No studies have adequately tested the effects of DMARDs on human outcomes, and so we have so far relied on observational data from incidental exposures. Until 1993, women of childbearing potential were excluded from randomised controlled trials. Although they are now eligible for inclusion in pharmaceutical trials, pregnancy is prohibited, noted as an ‘adverse effect’.
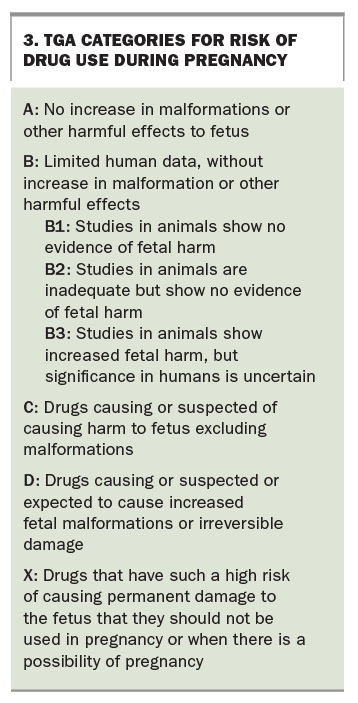
Shepard’s principles of teratology state that the agent must be present during crucial periods of development and that experimental models must corroborate findings (i.e. there must be biological plausibility, with the medication acting directly on embryo, fetus or placenta). In Australia, medications are classified according to the TGA categorisation of risk of drug use in pregnancy (Box 3). Unfortunately, the letters in this system are often misinterpreted as gradings. Patients, their families, allied health professionals and many doctors fail to grasp the relevant issues, and patients cease medications for unwarranted reasons.
{kind=link}
To avoid such problems in the USA, a pregnancy and lactation-labelling rule was implemented in 2015. This rule mandates removing all pregnancy letter categories from prescription medications in the next three to five years and replacing them with an integrated risk summary for use during pregnancy and lactation and for women and men with reproductive potential. To date, the TGA has no plans to modify the Australian procedure.
Optimising RA treatment in pregnancy
There is increasing evidence that some medications used to treat RA are compatible with pregnancy, whereas others are not. In light of the evidence that RA does not improve during pregnancy for all women and that active RA has potentially adverse outcomes for both the mother and baby, patients should be counselled about the use of medications during the preconception period, pregnancy and the postnatal period. Women of childbearing age with RA need a plan for possible pregnancy. It is also helpful to discuss management options with those who are not actively contemplating pregnancy, so that they are aware of them.
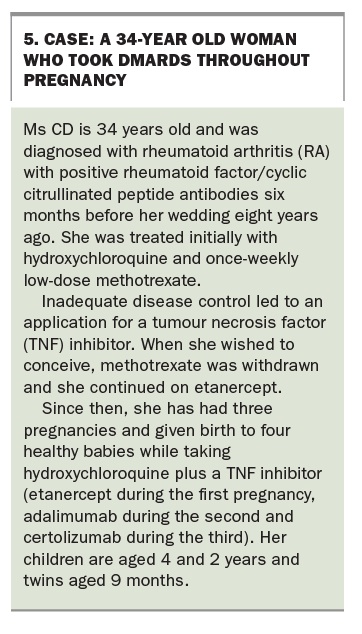
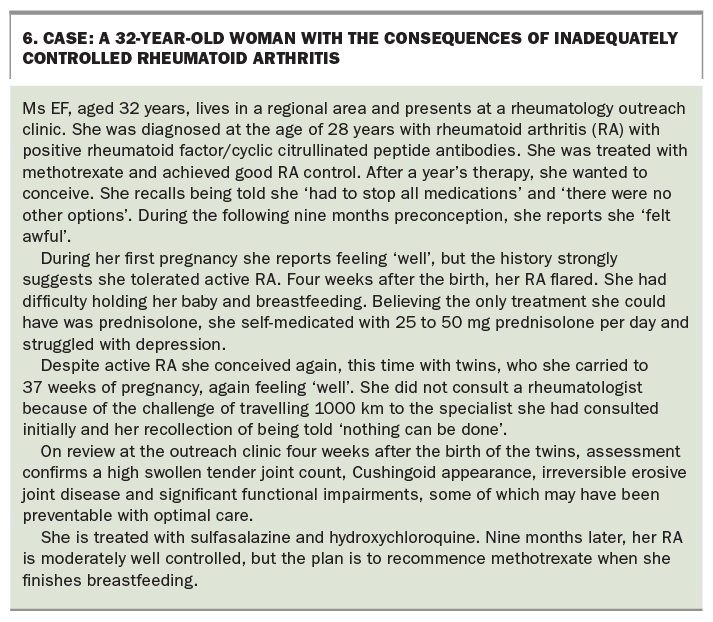
Recommendations on medication use in pregnancy are summarised in Box 4.12-15 Cases that illustrate the safe use of DMARDs throughout pregnancy and the consequences of inadequately controlled disease are described in Box 5 and Box 6, respectively.
{kind=link}
{kind=link}
{kind=link}
More details of medication TGA categories and recommendations for pregnancy, breastfeeding and paternal exposure are shown in Table 2.12-15
NSAIDs
Cessation of NSAIDs should be considered when conception is planned. Past reports on NSAIDs in the general population suggested the possibility of a low risk of miscarriage, but more recent studies do not support this finding. However, because of a possible adverse effect of NSAIDs on ovulation, a trial period off NSAIDs could be considered in women with a delayed time to pregnancy.
Selective cyclo-oxygenase (COX)-2 inhibitors should be avoided during pregnancy, as safety data are limited. If a nonselective NSAID other than low-dose aspirin is taken during pregnancy then it should be ceased at gestational week 32 to avoid premature closure of the ductus arteriosus. Low-dose aspirin may be continued throughout the pregnancy.
Glucocorticoids
Initial human studies on glucocorticoids in pregnancy reported an increased incidence of cleft palate in newborns, and this statement persists in the literature despite more recent findings that do not support the association.16 Prednisolone use by pregnant women with RA is associated with a higher risk of small-for-gestational-age infants. At doses higher than 7.5 mg per day, prednisolone is also associated with subfertility.3 In addition, the general adverse effects of corticosteroids (increased infection, weight gain, hypertension, diabetes and osteoporosis) are more common in pregnancy. Hence, use of prednisolone during pregnancy should be carefully considered and minimised when possible to reduce the risks to the mother and baby.
DMARDs
A full description of all DMARDs and their role in pregnant women with RA is beyond the scope of this article. Key points are highlighted below. More details are available in Prescriber’s Information on Medications for Rheumatic Diseases in Pregnancy from the Australian Rheumatology Association (http://www.rheumatology.org.au/gps/clinical-guidelines.asp).15
Hydroxychloroquine
Hydroxychloroquine is recommended for use during pregnancy because of strong evidence for its favourable risk–benefit profile.12 Nevertheless, its TGA pregnancy category is D, which can make patients and others needlessly anxious.
Sulfasalazine
Sulfasalazine (TGA category A) coprescribed with folate 5 mg daily (as sulfasalazine inhibits folate absorption) is recommended to treat women with RA before and during pregnancy.12
Methotrexate
Methotrexate is the first DMARD recommended in all international RA treatment guidelines because its benefits outweigh its risks. Methotrexate is not recommended in pregnancy but because of its frequency of use, exposure to low-dose methotrexate before or early in pregnancy has been reported. A study compared 324 women exposed to methotrexate around the time of conception (136 before and 188 after conception) with 459 disease-matched control subjects and 1107 control subjects without autoimmune disease. The incidence of major birth defects was not significantly different in the preconception exposure group (3.5%), disease-matched group (3.6%) and nonautoimmune disease group (2.9%), but was higher in the postconception exposure group (6.6%).17 No malformations consistent with methotrexate embryopathy were detected.
In the case of unplanned conception, the woman should cease taking methotrexate immediately while either continuing folate (5 mg daily) or using folinic acid (15 mg six-hourly for one day then eight-hourly for two days). Expert advice should be sought from a rheumatologist or obstetric medicine physician.
Limited evidence suggests that unplanned conception when the father is taking methotrexate is safe. In 113 pregnancies with paternal methotrexate exposure there was no increase in risk of adverse fetal outcomes compared with pregnancies in which fathers were not exposed.18
Leflunomide
A study of leflunomide in pregnancy showed no increase in adverse pregnancy outcomes among pregnant women who stopped taking leflunomide in the first trimester and followed the cholestyramine washout protocol (8 g three times daily for 11 days).19 In the case of unplanned conception, leflunomide should be stopped immediately and cholestyramine washout given until leflunomide plasma levels are undetectable. Expert advice should be sought.
Biological DMARDs
All patients with RA receiving biologic therapy and considering pregnancy (or found to be pregnant) should discuss their individualised management plan with their treating rheumatologist. Modes of action of biological DMARDs currently subsidised by the PBS for patients with severe active RA are listed in Table 3. With the exception of certolizumab, they are all large molecules with an IgG-like structure and, like other maternal immunoglobulins, are actively transported across the placenta from gestational week 16, with the transport rate increasing later in pregnancy up until birth. The exception, certolizumab, is a pegylated antibody molecule with a much lower transport rate across the placenta.
{kind=link}
Measurement of drug levels in cord blood of babies born of mothers taking tumour necrosis factor (TNF) inhibitors has shown high levels of adalimumab and infliximab but lower levels of etanercept and certolizumab.20 Analyses of large databases have shown no adverse pregnancy outcomes in pregnant women with RA or inflammatory bowel disease who were exposed to TNF inhibitors compared with the general population.21 However, a small prospective trial showed that cessation of TNF inhibitors in pregnancy was associated with an increased rate of flares.22 This finding was supported by a systematic review of data from more than 2000 pregnancies.23
Consequently, it is currently recommended to continue TNF inhibitor therapy during pregnancy when indicated. Paternal exposure to TNF inhibitors is also considered low risk.24 To limit exposure of the fetus, it is generally recommended that infliximab and adalimumab are withheld from gestational week 20 and restarted after the birth,25 with the decision reviewed in light of the clinical indications. Etanercept and certolizumab can be continued throughout pregnancy if clinically indicated.
Biological DMARDs with other modes of action cannot currently be recommended in pregnancy until further information is gathered. If exposures have occurred inadvertently then the pregnancy can continue, but expert opinion from both the rheumatologist and an obstetric medicine physician should be sought.
Breastfeeding is considered safe for women receiving biological DMARDs as these medications are unlikely to be absorbed by the baby, owing to digestion in the stomach. Avoidance of live vaccines for the first six months is recommended in neonates who have been exposed to biological DMARDs during the third trimester, other than certolizumab and etanercept, based on the death of an infant due to disseminated BCG infection after vaccination when infliximab had been continued throughout the pregnancy. Live vaccines recommended for infants aged under 6 months in Australia include rotavirus vaccine and (for specific indications) BCG.
Conclusion
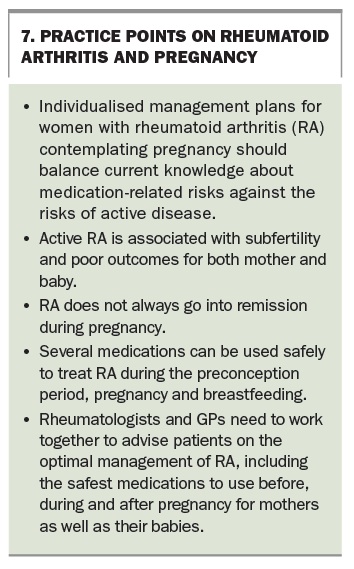
It is important to maintain optimal disease control in patients with RA who are planning pregnancy, are pregnant or have recently given birth, for the health of both the mother and the baby. Some practice points on RA and pregnancy are summarised in Box 7. A number of prescribed DMARDs are safe to continue during these times. Preconception discussion of management options should be part of routine clinical practice for all women of childbearing age with RA. This will help ensure successful outcomes for mother and baby.
COMPETING INTERESTS: Dr Barrett and Dr Young have received an unrestricted educational grant from UCB Pharma to support the Pregnancy Exposed to Biological (PEB) Study.
References
- Arthritis and Osteoporosis Victoria. A problem worth solving. Elsternwick: Arthritis and Osteoporosis Victoria; 2013.
- Australian Institute of Health and Welfare. Australia’s mothers and babies 2013 – in brief. Perinatal statistics series no. 31. Cat no. PER 72. Canberra: AIHW; 2015.
- Brouwer J, Hazes JM, Laven JS, Dolhain RJ. Fertility in women with rheumatoid arthritis: influence of disease activity and medication. Ann Rheum Dis 2015; 74: 1836-1841.
- Bermas BL, Sammaritano LR. Fertility and pregnancy in rheumatoid arthritis and systemic lupus erythematosus. Fertility Res Pract 2015; 1: 13.
- Skomsvoll JF, Ostensen M, Baste V, et al. Number of births, interpregnancy interval, and subsequent pregnancy rate after a diagnosis of inflammatory rheumatic disease in Norwegian women. J Rheumatol 2001; 28: 2310-2314.
- Barrett JH, Brennan P, Fiddler M, et al. Does rheumatoid arthritis remit during pregnancy and relapse postpartum? Results from a nationwide study in the United Kingdom performed prospectively from late pregnancy. Arthritis Rheum 1999; 42: 1219-1227.
- de Man YA, Dolhain RJ, van de Geijn FE, et al. Disease activity of rheumatoid arthritis during pregnancy: results from a nationwide prospective study. Arthritis Rheum 2008; 59: 1241-1248.
- Chakravarty EF, Nelson L, Krishnan E. Obstetric hospitalizations in the United States for women with systemic lupus erythematosus and rheumatoid arthritis. Arthritis Rheum 2006; 54: 899-907.
- Lin HC, Chen SF, Chen YH. Increased risk of adverse pregnancy outcomes in women with rheumatoid arthritis: a nationwide population-based study. Ann Rheum Dis 2010; 69: 715-717.
- Wallenius M, Salvesen KA, Daltveit AK, Skomsvoll JF. Rheumatoid arthritis and outcomes in first and subsequent births based on data from a national birth registry. Acta Obstet Gynecol Scand 2014; 93: 302-307.
- Demicheva, E, Crispi F. Long-term follow-up of intrauterine growth restriction: cardiovascular disorders. Fetal Diagn Ther 2014; 36: 143-153.
- Flint J, Panchal S, Hurrell A, et al; BSR and BHPR Standards, Guidelines and Audit Working Group. BSR and BHPR guideline on prescribing drugs in pregnancy and breastfeeding – Part I: standard and biologic disease modifying antirheumatic drugs and corticosteroids. Rheumatology (Oxford) 2016; 55: 1693-1697.
- Flint J, Panchal S, Hurrell A, et al; BSR and BHPR Standards, Guidelines and Audit Working Group. BSR and BHPR guideline on prescribing drugs in pregnancy and breastfeeding – Part II: analgesics and other drugs used in rheumatology practice. Rheumatology (Oxford) 2016; 55: 1698-1702.
- Ngian GS, Briggs AM, Ackerman IN, Van Doornum S. Safety of anti-rheumatic drugs for rheumatoid arthritis in pregnancy and lactation. Int J Rheum Dis 2016; 19: 834-843.
- Australian Rheumatology Association. Prescriber’s information on medications for rheumatic diseases in pregnancy. Revised ed. Sydney: ARA; 2016. Available online at: https://rheumatology.org.au/gps/clinical-guidelines.asp (accessed January 2017).
- Hviid A, Molgaard-Nielsen D. Corticosteroid use during pregnancy and risk of orofacial clefts. CMAJ 2011; 183: 796-804.
- Weber-Schoendorfer C, Hoeltzenbein M, Wacker E, et al. Pregnancy outcome after methotrexate treatment for rheumatic disease prior to or during early pregnancy. Arthritis Rheum 2014; 66: 1101-1110.
- Weber-Schoendorfer C, Hoeltzenbein M, Wacker E, et al. No evidence for an increased risk of adverse pregnancy outcome after paternal low-dose methotrexate: an observational cohort study. Rheumatology 2014; 53: 757-763.
- Chambers CD, Johnson DL, Robinson LK, et al. Birth outcomes in women who have taken leflunomide during pregnancy. Arthritis Rheum 2010; 62: 1494-1503.
- Mahadevan U, Wolf DC, Dubinsky M, et al. Placental transfer of anti-tumor necrosis factor agents in pregnant patients with inflammatory bowel disease. Clin Gastroenterol Hepatol 2013; 11: 286–292, quiz e224.
- Mahadevan U, Martin C, Sandler R, et al. PIANO: a 1000 patient prospective registry of pregnancy outcomes in women with IBD exposed to immunomodulators and biologic therapy. Gastroenterol 2012; 142 (5 Suppl 1): S-149.
- Fischer-Betz R, Sander O, Specker C, Brinks R, Schneider M. High risk of flares during pregnancy in women with rheumatoid arthritis who discontinue treatment with TNF inhibitors at conception. ACR Abstract No. 2522; 2015 ACR/ARHP Annual Meeting. Available online at: http://acrabstracts.org/abstract/high-risk-of-flares-during-pregnancy-in-women-with-rheumatoid-arthritis-who-discontinue-treatment-with-tnf-inhibitors-at-conception (accessed January 2017).
- Vinet E, Pineau C, Gordon C, Clarke AE, Bernatsky S. Biologic therapy and pregnancy outcomes in women with rheumatic diseases. Arthritis Rheum 2009; 61: 587-592.
- Puchner R, Danninger K, Puchner A, Pieringer H. Impact of TNF-blocking agents on male sperm characteristics and pregnancy outcomes in fathers exposed to TNF-blocking agents at time of conception. Clin Exp Rheum 2012; 30: 765-767.
- Gotestam Skorpen C, Hoetlzenbein A, Tincani A, et al. The EULAR points to consider for use of antirheumatic drugs before pregnancy, and during pregnancy and lactation. Ann Rheum Dis 2016; 75: 795-810.