The discharging ear. A good history tells the story

Ear infections
Ear disorders
- The discharging ear can represent a large variety of conditions that can occur in patients of any age.
- Taking a history is an essential part of the assessment of patients with ear pathology.
- Common causes of purulent or mucoid discharge include otitis externa, a foreign body, a cholesteatoma or otitis media with perforation of the tympanic membrane.
- Clear discharge is an uncommon form of otorrhoea in general practice. Usually the history indicates underlying aetiology.
- Blood-stained discharge usually causes significant concern to the patient. It has a range of possible causes from more benign pathology such as acute otitis media to more serious concerns such as middle ear or ear canal tumours.
- Classifying the type of discharge present allows the various common aetiologies to be considered, enabling accurate treatment or referral of the patient.
Picture credit: © pathdoc/stock.adobe.com
The discharging ear is a common presentation in general practice. It can represent a large variety of conditions that can occur in patients of any age group. A logical approach to assessment and diagnosis enables accurate treatment and/or referral of the patient.
Assessment
Taking a history is an essential part of the assessment of ear pathology. A significant number of conditions can be diagnosed based only on the history. The most obvious point is the type of discharge. There are three main types of discharge: purulent, clear and blood-stained discharge.
Other essential features include the presence or absence of otalgia, tenderness (particularly in the region of the tragus or mastoid), hearing loss, tinnitus (either pulsatile or constant) and vestibular disturbance. Other relevant facts to include in the assessment are rapidity of onset and time frame of the discharge, history of previous episodes, previous surgery, trauma (including use of cotton buds or earplugs), activities that involve flying or diving and dermatological conditions.
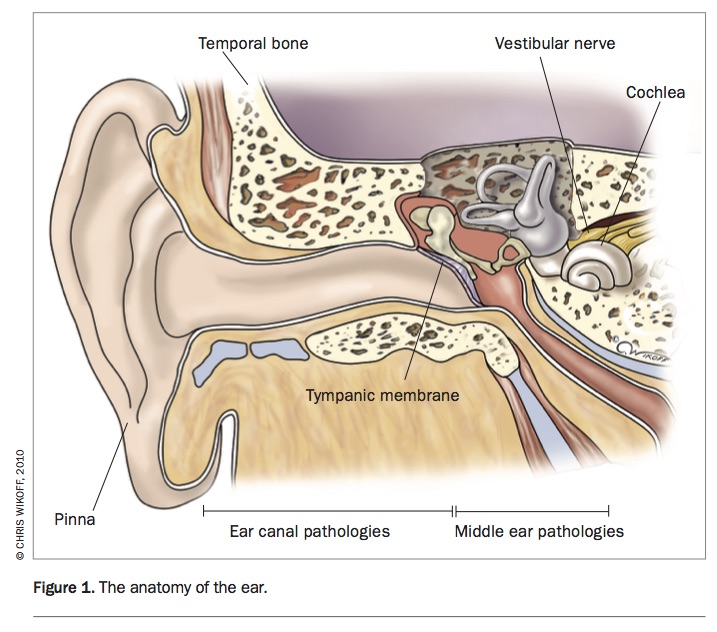
When examining a patient, it is important to have a good understanding of the anatomy of the ear and to consider the condition in respect to anatomical divisions (Figure 1).
{kind=link}
The first consideration is the state of the pinna and ear canal. After that, consider the state of the tympanic membrane, followed by the middle ear and, finally, hearing and vestibular function. Good visualisation is best achieved with the largest speculum available.
Type of discharge
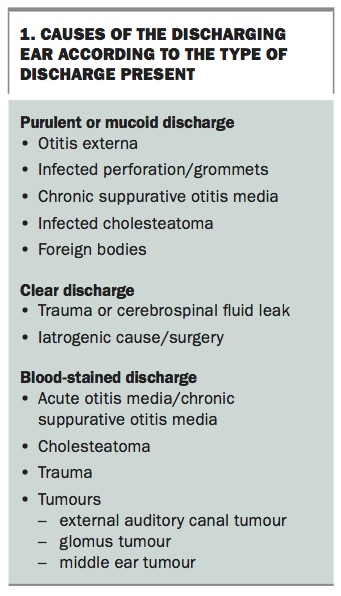
The type of discharge – purulent or mucoid, clear or blood stained – can indicate common diagnoses (Box 1). In broad terms, purulent or mucoid discharge is the most common type of discharge encountered. Clear discharge is relatively uncommon but can have significant implications. Blood-stained discharge can represent a wide range of conditions from benign pathology to malignancy.
{kind=link}
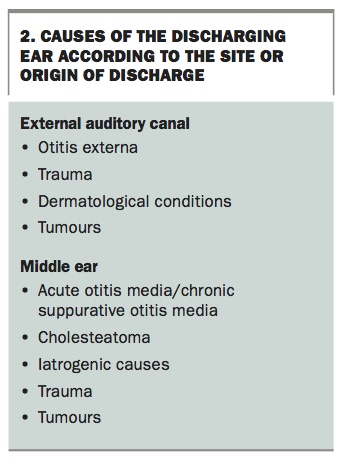
It is also possible to classify the discharge according to site or origin (Box 2). General discharge arises from either the external auditory canal or the middle ear. The inner ear is not considered as perilymph leaks from the cochlea are not usually of sufficient volume to present as a discharging ear.
{kind=link}
Purulent or mucoid discharge
Purulent or mucoid ear discharge can occur in any age group and can represent a variety of conditions. The most common cause of purulent or mucoid discharge from the ear canal is otitis externa.
Otitis externa
Acute otitis externa is often related to trauma of the ear canal or trapping of water within the ear canal. It comes in two forms. The most common form is bacterial, caused by infection with Staphylococcus or Pseudomonas species. Bacterial otitis externa classically presents with a rapidly evolving severe otalgia with extreme tenderness, particularly over the tragus, and swelling over the ear canal, which may extend into the pre- and postauricular regions. Severe tenderness on palpating the tragus is pathognomonic of bacterial otitis externa. Otoscopy often reveals severe oedema with mucopurulent exudate. Patients often find this examination extremely painful.
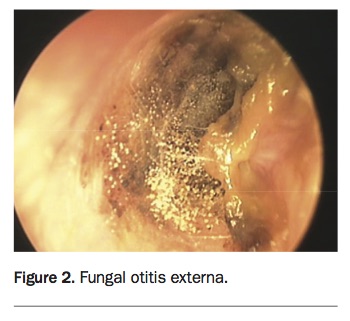
Fungal otitis externa is less common and often seen following the use of antibiotic medications within the ear canal (Figure 2). Antibiotics eliminate the normal bacterial flora within the ear canal, allowing a secondary fungal overgrowth. Aspergillus niger and Candida albicans are the two most commonly encountered fungal agents. Fungal otitis externa is often characterised by a more chronic indolent course with significant itch and less pain. Both types result in temporary conductive hearing loss. Fungal otitis externa is further characterised by the possibility of fungal erosion of the tympanic membrane resulting in perforation. In bacterial otitis externa, perforation is extremely rare.
{kind=link}
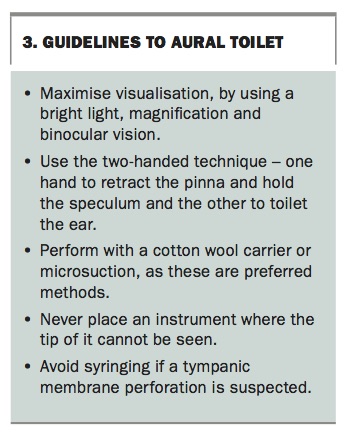
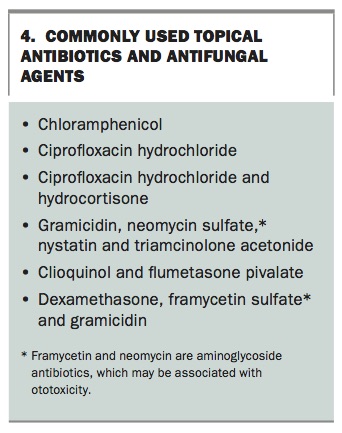
The key to treating otitis externa is removing underlying debris in the ear canal with aural toilet (Box 3), followed by application of topical antibiotic or antifungal drops (Box 4). Aural toilet is usually performed with dry swabs or micro- suction. Syringing of the ear is a less ideal treatment. An ear wick covered with a corticosteroid/antibiotic combination ointment is used when there is significant swelling. A swab may be taken for culture to direct the choice of antibiotic. The patient should keep the ear dry until the condition has completely resolved.
{kind=link}
{kind=link}
For patients with recurrent otitis externa, preventive techniques, such as use of ear plugs to avoid water exposure and alcohol-based drops after water exposure, are recommended. Predisposing factors such as severe exostoses can be addressed surgically to help combat recurrent episodes.
Otitis externa is a much more serious condition in people who are immunocompromised or who have diabetes. This group of patients has an increased risk of developing malignant otitis externa (skull base osteomyelitis). This condition is characterised by ongoing pain and discharge that fails to respond to standard treatments. A high index of suspicion is required. Pseudomonas spp. is a common aetiological agent, although fungal infections are also recognised. Intensive antibiotic or antifungal therapy is required, usually for a minimum of six weeks and often for up to three months. This condition can progress, causing multiple cranial nerve palsies. There is a significant mortality associated with malignant otitis externa.
Foreign bodies
Patients – often young children – who have foreign bodies in the ear canal may present with a purulent or mucoid discharge. The foreign body may be organic or inorganic. Inorganic materials, such as beads, generally do not produce a significant inflammatory response unless there has been trauma to the skin of the ear canal in the process of placing the foreign body. Foreign bodies need to be carefully removed, particularly in small children. This requires a two-handed technique to avoid traumatising the ear canal if the head moves. When removing a foreign body, it is essential to completely visualise the foreign body under binocular magnification so that any instrument used does not traumatise the tympanic membrane. Often small children require sedation or a general anaesthetic to enable removal of foreign bodies deep in the ear canal. Attempting to remove a foreign body with glue on a ridged object is not generally recommended unless there is no alternative means of removal.
Acute otitis media
Middle ear pathologies such as acute otitis media also commonly present with purulent or mucoid discharge. This common condition is usually caused by bacterial infection and often presents with typical features of otalgia, fever, malaise and then a secondary blood-stained purulent discharge that signifies spontaneous perforation of the tympanic membrane. These perforations are minute and usually resolve within 24 to 48 hours. Uncommonly they may persist and a more permanent perforation may evolve. Spontaneously discharging acute otitis media is treated with oral antibiotics, such as amoxycillin.
Infected grommets
Infected grommets (ventilating tubes) are a common cause of a purulent discharge. Pain is not a common feature of this condition, which involves a range of bacterial agents, including Staphylococcus spp. and Gram-negative bacteria such as Pseudomonas spp. Treatment is best undertaken with aural toilet and topical antibiotics. With recent increasing concern over aminoglycoside ototoxicity, topical antibiotics can be limited to the quinolone class to avoid this risk.1 Oral antibiotics are occasionally used in severe cases or when there is a lack of initial response to topical antibiotic drops.
Chronic suppurative otitis media
Chronic suppurative otitis media needs to be considered when a purulent, mucoid or blood-stained discharge persists for a few months. This condition can occur in any age group. A common predisposing feature is Eustachian tube dysfunction. The presentation usually consists of recurrent or constant otorrhoea with minimal otalgia. A range of pathogens can cause this condition. Gram-negative agents such as Pseudomonas spp. and Escherichia coli are common. Otoscopic findings include a tympanic membrane perforation, myringitis, granulation tissue or infection. This condition requires significant intervention with both antibiotics and surgery. The potential complications of this condition are serious, including permanent hearing loss of a conductive and sensorineural nature, mastoiditis, facial nerve injury and meningitis.2
Cholesteatoma
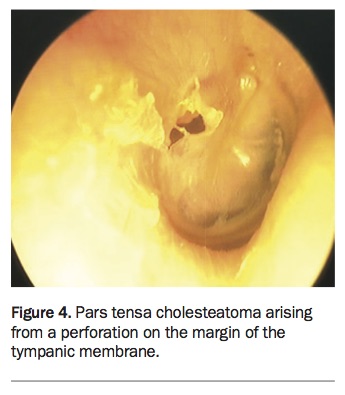
Cholesteatoma often presents with a continually discharging ear. This locally destructive condition is an abnormal ingrowth of squamous epithelium from the tympanic membrane. It may arise from the pars flaccida or pars tensa. Pars flaccida cholesteatoma usually erodes superiorly over the head of the malleus into the epitympanum and through into the mastoid air cell system (Figure 3). Pars tensa cholesteatoma often arises from a perforation on the margin of the tympanic membrane (Figure 4). Squamous epithelium may migrate down from the margin of the tympanic membrane into the meso-tympanum over the ossicular chain and again into the mastoid air cell system. Cholesteatoma presents with intermittent or continued purulent, mucoid or blood-stained discharge despite treatment. A high index of suspicion is required in this situation. Patients with a long history of chronic ear problems may develop this condition.
{kind=link}
{kind=link}
Treatment of cholesteatoma is surgical; the extent of the mastoidectomy is determined by the degree of the cholesteatoma. Complications of cholesteatoma are serious and include conductive and sensorineural hearing loss, mastoiditis, labyrinthitis, facial nerve injury, meningitis and cerebrospinal fluid (CSF) leak.
Clear discharge
Clear discharge is an uncommon form of otorrhoea in general practice. Usually the history indicates the underlying aetiology. Trauma to the ear canal or tympanic membrane may present with a haemo- serous or clear discharge. The use of cotton buds or a direct blow to the ear are common causes.
Head injury
A clear ear discharge in a patient with a history of significant head injury is a more serious concern. Clear otorrhoea following such an event should always raise the suspicion that the otorrhoea is CSF. Temporal bone fractures are often missed on routine radiology. They are classified according to the involvement of inner-ear structures. The fractures may run through the roof of the middle ear or bony ear canal resulting in a direct leak of CSF through the ear canal. Such a presentation requires immediate referral for management and possible surgical repair of the leak. A clear discharge is also sometimes encountered after any ear or cranial surgical intervention. Usually, this intervention is evident on history and examination.
Blood-stained discharge
A blood-stained ear discharge usually causes significant concern to the patient. It has a range of possible causes, from the more benign pathology of acute otitis media through to more serious concerns, such as middle ear or ear canal tumours. It is important to note that otitis media – either acute or chronic – or cholesteatoma are by far the most common potential aetiologies.
Barotrauma
Barotrauma is also a potential cause of a blood-stained ear discharge and is a common presentation in general practice. It is caused by pressure changes, usually associated with flying or scuba diving. Water skiing and surfing are also recognised causes. Barotrauma can damage the tympanic membrane or middle ear and, rarely, the cochlea.
Tympanic membrane injury is usually characterised by initial pain, typically on descent, which may result in mild hearing loss but no ongoing vestibular symptoms. Severity can range from a simple haemorrhage into the layers of the tympanic membrane, to middle ear effusion or rarely tympanic membrane perforation. Tympanic membrane injury usually resolves spontaneously, although a course of antibiotics is often given if an effusion is present. Ventilating tubes can be useful in preventing repeated barotrauma.
Perilymphatic fistula is a rare form of barotrauma that involves rupture of the round or oval window membrane, allowing perilymph to escape from the cochlear and vestibular system and air to ingress. This results in acute onset of sensorineural hearing loss, tinnitus and vertigo. It requires immediate treatment with corticosteroids and surgical repair and is considered a surgical emergency.
Direct trauma
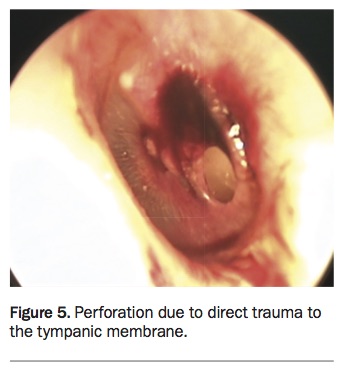
Direct trauma can also occur to the tympanic membrane, usually relating to a foreign body such as a cotton bud (Figure 5). Initial pain usually occurs associated with hearing loss, but vestibular dysfunction is uncommon. About 80 to 90% of traumatic perforations will heal, unless secondary infection becomes established. Ongoing vestibular symptoms should raise a suspicion of perilymphatic fistula.
{kind=link}
Direct trauma such as a head injury may result in a fractured temporal bone. Fractures of the temporal bone and skull base often present with blood-stained otorrhoea or haemotympanum. The sequelae can be severe, particularly if the fracture line crosses the cochlear or vestibular system resulting in a ‘dead ear’ (total hearing loss), as well as severe vertigo. Other associated features can include facial nerve palsy, CSF leak or meningitis. Haemotympanum is usually managed conservatively, as are many fractures of the temporal bone, unless an active CSF leak is present.3
Tumours
In rare instances, purely blood-stained discharge of the ear can represent a tumour, which may be benign or malignant. The most common malignancy in the ear is a squamous cell carcinoma.4 Basal cell carcinomas are also recognised and in rare instances minor salivary gland tumours may arise in the cartilaginous canal.
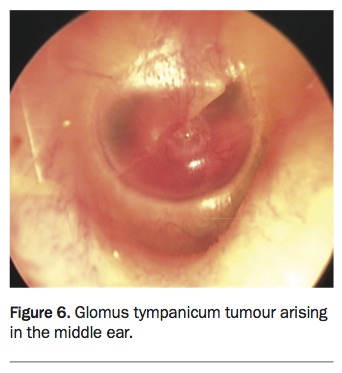
Glomus tumours (also known as para-gangliomas), which are related to carotid body tumours, can also arise in the middle ear (Figure 6). These rare tumours are highly vascular and when large may penetrate the tympanic membrane and lead to a blood-stained discharge. Treatment for these complex conditions is difficult and patients are usually managed in a tertiary referral skull base unit.
{kind=link}
Conclusion
The discharging ear is a common presentation in general practice and can represent a large variety of conditions. A simple form of classifying the discharge allows the various common aetiologies to be considered, enabling accurate treatment or referral of the patient. MT