Reducing cardiovascular risk in type 2 diabetes: can we do more?

Heart diseases
Diabetes type 2
Results of recent cardiovascular outcome studies have shown significant reductions in cardiovascular disease and overall mortality using sodium–glucose cotransporter-2 inhibitors and glucagon- like peptide-1 receptor agonists and have made us rethink our choices of pharmacotherapy. These agents should now be considered earlier in the management of patients with type 2 diabetes to reduce cardiovascular risk, particularly in those with existing cardiovascular disease.
- Type 2 diabetes is associated with a significant increase in cardiovascular risk.
- Early glycaemic control reduces microvascular complications that in the long term may also translate to decreased macrovascular complications.
- Traditional antihyperglycaemic agents do not appear to have any specific beneficial cardiovascular effects, with the possible exception of metformin.
- More recently, some trials have shown significant reductions in cardiovascular and overall mortality using sodium–glucose cotransporter-2 (SGLT-2) inhibitors and glucagon-like peptide-1 receptor agonists in specific patient populations, particularly in those with established cardiovascular disease.
- SGLT-2 inhibitors may also reduce hospitalisation with heart failure.
- These agents should now be considered earlier in the management of patients with type 2 diabetes to reduce cardiovascular risk, particularly in those with existing cardiovascular disease.
- Management of each patient should be individualised; if these newer agents are used, the relative benefits and potential side effects should always be discussed with the patient.
Picture credit: © milatas/stock.adobe.com Model used for illustrative purposes only
The prevalence of type 2 diabetes continues to rise because of a combination of factors, particularly the ever increasing rate of obesity, but also longer life expectancy and increased vigilance in screening and detection. It has been well established that type 2 diabetes is associated with an increase in premature cardiovascular complications and mortality. Traditional antihyperglycaemic agents have had no clear impact on decreasing cardiovascular risk, but early glycaemic control lowers the rate of cardiovascular mortality in the long term.1,2
Newer therapies, namely the sodium–glucose cotransporter-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists, address some of the complex pathophysiological abnormalities associated with diabetes and have lower rates of hypoglycaemia and weight gain. In recent cardiovascular outcome studies, these two drug classes have also shown beneficial cardiovascular effects, including reductions in cardiovascular death in patients with established cardiovascular disease taking empagliflozin and patients at high risk of cardiovascular disease taking liraglutide.3,4
One of the goals in the management of diabetes must be to reduce diabetes-related death and macrovascular and microvascular complications. Management entails much more than just lowering blood glucose levels and cannot focus solely on glycaemic control. A multifactorial approach toward lowering cardiovascular risk is essential and should include targets such as lipid levels and blood pressure. This multifactorial approach has been shown to have significant benefits.5
More recently, the results of cardiovascular outcome studies evaluating the safety of the newer pharmacological agents have expanded the focus of management to include the potential beneficial nonglycaemic effects of these agents.3,4 This article focuses on the effects of antihyperglycaemic medications on cardiovascular disease; however, this focus in no way discounts the profound effects of diabetes on microvascular and other complications.
Epidemiology of diabetes and cardiovascular disease
A global problem
About 387 million people worldwide, or 8.3% of adults, have type 2 diabetes.6 By 2035 about 592 million people, or one in 10 adults, will have type 2 diabetes.6 In 2014, type 2 diabetes led to the deaths of about 4.9 million people, which equates to a person dying from type 2 diabetes-related conditions every seven seconds.6 Globally, type 2 diabetes is associated with a 1.76-fold relative increased risk of death from cardiovascular disease and a 2.26-fold increased risk of stroke.7
An Australian problem
In Australia, cardiovascular disease is estimated to account for more than 80% of deaths in people with type 2 diabetes.8 On average, a 60-year-old of either sex with type 2 diabetes but no history of cardiovascular disease would die about six years younger than their counterpart without type 2 diabetes. A 60-year-old of either sex with both type 2 diabetes and a history of cardiovascular disease would die about 12 years earlier than someone without either condition.9,10
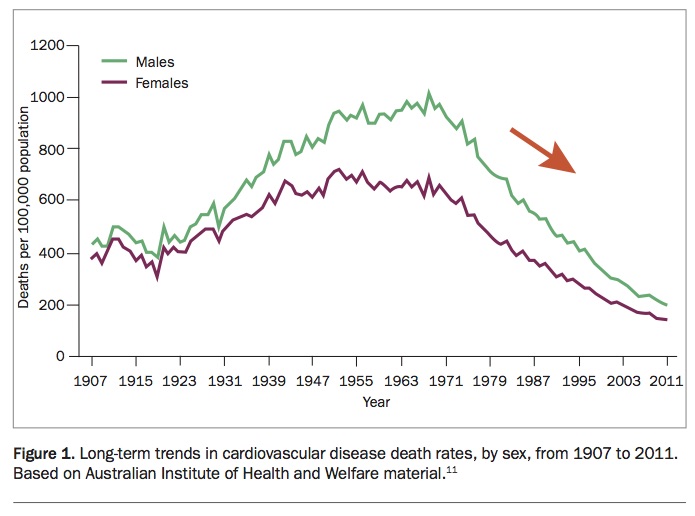
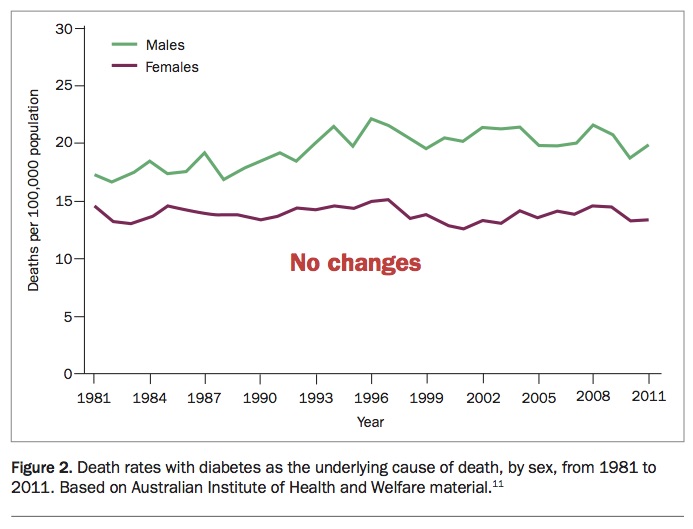
In the general population, cardiovascular mortality in Australia has been decreasing since its peak in 1968, when adjusted for age and population growth (Figure 1).11 However, the rate of cardiovascular deaths associated with type 2 diabetes has not changed in the past 30 years (Figure 2).11 Moreover, the number of patients with type 2 diabetes dying from cardiovascular disease has significantly increased in the past 10 years.12
{kind=link}
{kind=link}
Therapies for improving cardiovascular survival in people with type 2 diabetes
Agents that reduce cardiovascular risk in patients with or without diabetes include those that lower LDL-cholesterol levels and those that control blood pressure, in particular, agents that act on the renin–angiotensin system. These agents are becoming standard adjunct therapy for patients with type 2 diabetes because of the effects of these drugs on cardiovascular and overall mortality.
Statins
As most deaths in patients with type 2 diabetes are caused by cardiovascular disease, management focused on preventing death from cardiovascular disease should be paramount in these patients.8 Statins remain the clear first-line choice when starting drug therapy. The results of several systematic reviews have consistently suggested that people with type 2 diabetes gain at least similar benefits from statin therapy as those without type 2 diabetes.8
Antihypertensive therapy
For patients with type 2 diabetes, there is clear evidence that antihypertensive therapy with an ACE inhibitor, or an angiotensin II receptor blocker (ARB) if intolerant to ACE inhibitors, decreases the rate of progression of albuminuria, promotes regression to normoalbuminuria and may reduce the risk of decline in renal function.8 Combining an ARB and an ACE inhibitor is not recommended.13 ACE inhibitors and ARBs have made a significant difference in reducing the risk of cardiovascular disease in patients with type 2 diabetes and are now part of standard care for these patients.8
Intensive glycaemic control
The UK Prospective Diabetes Study (UKPDS) 33 assessed the efficacy of intensive glycaemic control compared with conventional therapy in patients with newly diagnosed or short-duration diabetes.14 The median glycated haemoglobin (HbA1c) level over 10 years was 7.0% in the intensive glycaemic control group and 7.9% in the conventional therapy group. Although no statistical difference was found in any macrovascular endpoint between intensive glycaemic control and conventional therapy over the 10-year period, there was a significant reduction in microvascular complications, such as retinopathy requiring photocoagulation, vitreous haemorrhage and renal failure.14 Moreover, in the 10-year follow up of UKPDS, there were fewer macrovascular complications in those who had been initially randomly assigned to the intensive glycaemic control group. These results have raised the concept of the ‘legacy effect’, indicating that early targeting of glycaemic control may translate to fewer cardiovascular complications in the long term.
The UKPDS 33 results contrast with those of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) study, the Veterans Affairs Diabetes Trial (VADT) and the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified-Release Controlled Evaluation (ADVANCE) trial, in which subjects had diabetes of longer duration with established complications and comorbidities.15-17
In these populations, aggressive glycaemic control had no clear benefit in decreasing further cardiovascular events. A meta-analysis of randomised trials evaluating more intensive (compared with less intensive) glycaemic control in patients with type 2 diabetes did not demonstrate a benefit for all-cause mortality (hazard ratio [HR], 1.04; 95% confidence interval [CI], 0.90 to 1.20) or cardiovascular death (HR, 1.10; 95% CI, 0.84 to 1.42).18
The lesson learned from these studies is that type 2 diabetes should not be regarded as a homogeneous entity. Patients should be ‘staged’ as far as age, comorbidities, duration of diabetes and life expectancy.19,20 Early intensive glycaemic control appears to reap benefits, but later aggressive treatment does not.
Lifestyle modification
The Action for Health in Diabetes (Look AHEAD) trial investigated the effects on cardiovascular risk factors of an intensive lifestyle intervention aimed at body weight reduction, compared with diabetes support and education (control group), in overweight or obese patients with type 2 diabetes.21 After one year, the intensive lifestyle intervention was associated with significantly higher proportions of patients achieving target HbA1c levels, blood pressure targets, and combined HbA1c targets, blood pressure targets and LDL-cholesterol goals. Although there was no effect of the intensive lifestyle intervention on cardiovascular risk after 9.6 years,21 the use of antihypertensive medications, statins and insulin was lower in the intervention group than in the control group.21 In addition, the wider benefits of lifestyle modification should not be underestimated and, in this study, they included benefits on quality of life and sleep.
Effects of existing antihyperglycaemic medications on cardiovascular mortality
Metformin
In UKPDS 34, metformin was compared with conventional therapy and found to significantly reduce myocardial infarction (MI), coronary deaths and all-cause mortality by 39%, 50% and 36%, respectively, in patients with newly diagnosed type 2 diabetes and low cardiovascular disease risk, whose body weight was more than 120% of their ideal weight.22 In the 10-year follow up of UKPDS, obese patients with type 2 diabetes treated with metformin continued to show a reduction in MI and death from any cause. However, the sample size in this study was small (n=342) and the participants were overweight or obese. Further, as this study was published in 1998, the lack of lipid-lowering drugs and blood pressure and kidney-preserving drugs that are now available potentially diminishes the relevance of this observation for present-day treatment.1 Intriguingly, metformin added to sulphonylurea compared with sulphonylurea alone was associated with an increased risk of diabetes-related death.22
The potential effects of metformin on cardiovascular risk factors require further assessment but may include improved lipid profiles, anti-atherogenic effects, decreased ischaemic injury and amelioration of oxidative stress.23,24 Other actions of metformin include alteration of bile acid recirculation and gut microbiota, resulting in enhanced enteroendocrine hormone secretion, and a small increase in GLP-1 levels.25
Sulphonylureas
To date, sulphonylureas have not been shown to reduce cardiovascular risk. These medications increase the risk of weight gain and hypoglycaemia – two adverse effects that are associated with increased cardiovascular disease risk.26 A meta-analysis has included all randomised controlled trials with a duration of 24 weeks or more of sulphonylurea use compared with use of nonsulphonylurea agents in patients with type 2 diabetes.27 There was variability among the included trials, but overall the risk of major adverse cardiovascular events was not increased in patients treated with sulphonylureas compared with other agents (p=0.52). However, the authors concluded that the cardiovascular safety of sulphonylureas could not be established unless evaluated in long-term cardiovascular outcome trials.
Thiazolidinediones
Thiazolidinediones (peroxisome proliferator-activated receptor-γ agonists) are used elsewhere but not widely in Australia, where several alternatives are available. Thiazolidinediones can increase body weight and the risk of congestive heart failure, especially in patients with diastolic dysfunction (p=0.07).28,29
Two separate meta-analyses for rosiglitazone and pioglitazone suggest potentially differing cardiovascular effects of these two thiazolidinediones.28,29 Compared with controls, rosiglitazone was associated with a significantly increased risk of MI and an increased risk (of borderline significance) of cardiovascular-related death.28 By contrast, there was a tendency towards a lower incidence of MI (HR, 0.81) or death (HR, 0.92) with pioglitazone.29 Pioglitazone was also associated with a significantly lower risk of the composite primary endpoint of death, MI or stroke but a significantly increased risk of serious heart failure.29 (The US Food and Drug Administration initially issued a ‘black box’ warning for rosiglitazone but, on the basis of a recent review of the clinical trials, lifted its restriction on the drug.29)
Dipeptidyl peptidase-4 inhibitors
Several mechanistic studies have indicated potential cardiovascular effects of dipeptidyl peptidase-4 (DPP-4) inhibitors, including a possible reduction in MI size in animals pretreated with a DPP-4 inhibitor;30,31 improved endothelium-dependent vasodilatation;32 antioxidant and anti-inflammatory properties, independent of glucose lowering;33 reduced atherosclerotic lesions;34 improved left ventricular function after MI;35,36 and improved postprandial plasma triglyceride levels.37 However, large cardiovascular outcome studies to date indicate that this class of agents appears to be safe overall but with no cardiovascular benefits compared with placebo.38-40
Intriguingly, the Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus – Thrombolysis in Myocardial Infarction (SAVOR-TIMI) 53 trial reported an increased risk of admission to hospital for heart failure in those with a history of heart failure (HR, 1.27) with use of the DPP-4 inhibitor saxagliptin.38 The Examination of Cardiovascular Outcomes with Alogliptin versus Standard of Care (EXAMINE) trial, which tested alogliptin in patients with type 2 diabetes and acute coronary syndrome, and the Trial Evaluating Cardiovascular Outcomes with Sitagliptin (TECOS) reported no significant effect on hospital admission for heart failure.39,40 Evidence from observational studies has been inconsistent. However, it is reassuring that the TECOS study comprised a significant number of older (mean age, 66 years; median duration of diabetes, 10 years) participants, in whom the use of sitagliptin appeared to be safe.
Antihyperglycaemic medications that improve cardiovascular outcomes
SGLT-2 inhibitors
Cardiovascular risk factors beyond glucose levels that can potentially be modulated with SGLT-2 inhibitors include blood pressure, weight, visceral adiposity, hyperinsulinaemia, arterial stiffness, albuminuria, circulating uric acid levels, oxidative stress, cardiorenal effects, cardiac oxygen demand, cardiac function and lipid levels (Figure 3).41 Three drugs in this class have been registered in Australia (canagliflozin, dapagliflozin and empagliflozin). Cardiovascular outcome trials have been published in the case of canagliflozin and empagliflozin, whereas the trial for dapagliflozin is ongoing.
{kind=link}
The EMPA-REG Outcome trial
The Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG Outcome trial) was the first study of a antihyperglycaemic agent in which participants treated with empagliflozin had improved rates of survival.3 This trial enrolled 7020 adults with type 2 diabetes and an average age of 63 years; 57% had type 2 diabetes for more than 10 years. Importantly, all patients had established cardiovascular disease (previous MI, 47%; coronary artery disease, 76%; stroke, 23%; and unstable angina or occlusive peripheral arterial disease, 21%), with 10% having a history of heart failure. Patients were excluded if they had severe renal impairment (estimated glomerular filtration rate [eGFR], <30 mL/min/1.73 m2). Participants were randomly assigned to receive empagliflozin 10 mg/day, empagliflozin 25 mg/day or placebo on a background of standard antidiabetic therapy.
It is also important to note that patients were well treated with respect to their established cardiovascular disease status: 81% were taking lipid-lowering therapy, 95% were taking antihypertensive therapy and 89% were taking antiplatelet or anticoagulant therapy.3 Almost half were taking insulin. Results included a 38% reduction in cardiovascular mortality and 32% reduction in all-cause mortality with empagliflozin compared with placebo. Other outcomes included a 35% reduction in hospitalisation for heart failure, as well as favourable effects on renal markers. These benefits were associated with a decrease of 0.6% in HbA1c levels, 2.5kg in weight loss and a reduction of 5.2 mmHg in systolic blood pressure.
The intriguing finding was that many of these results were evident within six months and often within three months.3 It is not clear exactly what led to the benefits in the EMPA-REG Outcome trial. However, decreases in blood pressure, uric acid levels, heart rate and/or sympathetic tone, and improvements in oxidative capacity (by producing adenosine triphosphate from ketone bodies, such as beta-hydroxybutyrate), endothelial function and cardiac function via natriuresis all might have contributed. The impact of lower use of sulphonylurea or insulin therapy (agents which may increase weight and possibly have deleterious effects) also remains to be elucidated.
The CANVAS program
The Canagliflozin Cardiovascular Assessment Study (CANVAS) program integrated data from two trials involving a total of 10,142 participants with type 2 diabetes and high cardiovascular risk.42 Participants in each trial were randomly assigned to receive canagliflozin (100mg/day with optional uptitration to 300mg/day) or placebo and were followed for a mean of 188.2 weeks. The primary outcome was a composite of death from cardiovascular causes, nonfatal MI or nonfatal stroke. The mean duration of diabetes was 13.5 years. A history of cardiovascular disease was seen in 65.6% of participants. The rate of the primary outcome was lower with canagliflozin than with placebo (occurring in 26.9 vs 31.5 participants per 1000 patient-years; HR, 0.86; 95% CI, 0.75 to 0.97; p<0.001 for noninferiority; p=0.02 for superiority).
On the basis of the prespecified hypothesis testing sequence, the renal outcomes were not viewed as statistically significant, but the results showed a possible benefit of canagliflozin with respect to the progression of albuminuria (HR, 0.73; 95% CI, 0.67 to 0.79). In addition, there was a 40% reduction in the eGFR, the need for renal replacement therapy or death from renal causes (HR, 0.60; 95% CI, 0.47 to 0.77) in those treated with canagliflozin. Intriguingly, there was an increased risk of amputation (6.3 vs 3.4 participants per 1000 patient-years; HR, 1.97; 95% CI, 1.41 to 2.75), which occurred primarily at the level of the toe or metatarsus.
GLP-1 receptor agonists
Three GLP-1 receptor agonists (exenatide, extended-release exenatide and liraglutide) are currently available in Australia. Cardiovascular outcome trials have been completed evaluating the safety of extended-release exenatide and liraglutide as well as two other compounds that are not available in Australia at this time: lixisenatide (trial indicated no effects on cardiovascular outcomes) and semaglutide (decreased composite outcome).43,44 These medications may modulate cardiovascular risk factors by a variety of mechanisms.45
LEADER trial
The Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial studied the cardiovascular effect of the GLP-1 receptor agonist liraglutide, when added to standard care for patients with type 2 diabetes.4 Patients with type 2 diabetes and high cardiovascular risk were randomly assigned to receive liraglutide (0.6 to 1.8 mg/day) or placebo. The major inclusion criteria were one of the following.
- an age of 50 years or more with at least one cardiovascular coexisting condition such as coronary heart disease, cerebrovascular disease, peripheral vascular disease, chronic kidney disease (stage 3 or greater) or chronic heart failure
- an age of 60 years or more with at least one cardiovascular risk factor, as determined by the investigator.
The primary composite outcome in the time-to-event analysis was the first occurrence of death from cardiovascular causes, nonfatal MI or nonfatal stroke. A total of 9340 patients were randomised and the median follow up was 3.8 years. The primary outcome occurred in significantly fewer patients in the liraglutide group (13%) compared with the placebo group (14.9%) (HR, 0.87; 95% CI, 0.78 to 0.97; p<0.001 for noninferiority; p=0.01 for superiority). Fewer patients died from cardiovascular causes in the liraglutide group (4.7%) than in the placebo group (6.0%; HR, 0.78; 95% CI, 0.66 to 0.93; p=0.007). The rates of nonfatal MI, nonfatal stroke and hospitalisation for heart failure were nonsignificantly lower in the liraglutide group than the placebo group.
EXSCEL
In the Exenatide Study of Cardiovascular Event Lowering (EXSCEL), patients with type 2 diabetes, with or without previous cardiovascular disease, received subcutaneous injections of extended-release exenatide 2mg or matching placebo once weekly.46 The primary composite outcome was the first occurrence of death from cardiovascular causes, nonfatal MI or nonfatal stroke. Of 14,752 patients, 73.1% had previous cardiovascular disease. Patients were followed for a median of 3.2 years. A primary composite outcome event occurred in 11.4% of patients in the exenatide group and 12.2% in the placebo group. The intention-to-treat analysis indicated that exenatide, administered once weekly, was noninferior to placebo with respect to safety but was not superior to placebo with respect to efficacy. The rates of death from cardiovascular causes and hospitalisation for heart failure did not differ between the groups.
Conclusion
Until recently, goals in the management of patients with type 2 diabetes have included:
- achieving an LDL-cholesterol level of less than 2.0mmol/L, a serum triglyceride level of less than 1.7mmol/L and an HDL-cholesterol level of more than 1.0mmol/L, preferably using statins
- achieving a systolic blood pressure of 130 to 140mmHg,20 preferably using ACE inhibitors (or ARBs if intolerant to ACE inhibitors), and
- individualising HbA1c targets.8
However, the results of the recent cardiovascular outcome studies have made us rethink our choices of pharmacotherapy. Drug classes such as SGLT-2 inhibitors and GLP-1 receptor agonists lower glucose levels and, when combined with metformin, have a low propensity for causing hypoglycaemia.
The aims of treating a patient with type 2 diabetes with or without pre-existing cardiovascular disease should include decreasing the risk of premature mortality, reducing complications and improving quality of life. It appears that, although the SGLT-2 inhibitors and GLP-1 receptor agonists are medications that lower blood glucose levels, they can also be regarded as potential cardiovascular medications at least in the patient groups studied in the cardiovascular outcome trials discussed; that is, those with established cardiovascular disease or who are at high cardiovascular risk.
When interpreting the results of these studies, the clinician will also need to determine if each patient’s particular characteristics, such as age, duration of diabetes and presence of pre-existing cardiovascular disease, are consistent with those of the subjects in each cardiovascular outcome trial. There is little doubt that the results of the recent cardiovascular outcome trials will potentially change the way in which clinicians will use pharmacological agents. However, there is not a more complex and heterogeneous chronic disease than type 2 diabetes. As clinicians, we must continue to formulate a unique and individual management plan including the choice of pharmacotherapy for each patient, taking into account the patient characteristics and results of the cardiovascular outcome trials rather than generically prescribing medications. MT