Atrial fibrillation and concomitant CAD: an individualised approach to combined antithrombotic therapy

Atrial fibrillation
Coronary artery disease
An individualised approach to antithrombotic management should be adopted in patients with atrial fibrillation and concomitant coronary artery disease with consideration to both bleeding and thrombotic risk.
- One in five patients receiving long-term anticoagulation have coronary artery disease.
- These patients present a unique challenge in balancing the risks and benefits of combined anticoagulant and antiplatelet therapies.
- The efficacy and safety of combination antiplatelet and anticoagulant therapies have been assessed recently in several trials.
- An individualised approach to antithrombotic management should be adopted in patients with dual indications, typically those with pre-existing nonvalvular atrial fibrillation presenting with an acute coronary syndrome, with consideration to both bleeding and thrombotic risks.
Current guidelines on atrial fibrillation (AF) suggest an individualised antithrombotic strategy based on assessment of thrombotic and bleeding risks.1 Patients with a high risk of stroke invariably have a high risk of major bleeding, although the net clinical benefit usually favours stroke prevention.1
Stroke risk assessment: CHA2DS2-VASc score
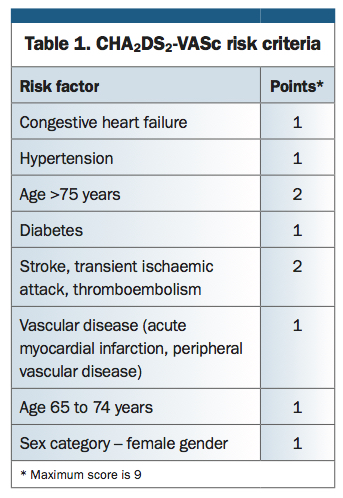
International guidelines strongly recommend initiating anticoagulation in patients with nonvalvular AF and a CHA2DS2-VASc score of 2 or greater, where the adjusted annual stroke rate is more than 2%. The guidelines also recommend considering anticoagulation in patients with a CHA2DS2-VASc score of 1 (annual stroke rate of 1.3%) provided there are no major contraindications to anticoagulation (Table 1 and Table 2).2
{kind=link}
{kind=link}
Recent studies suggest female gender is a stroke risk modifier rather than an overall or specific risk factor.3 This concept is reflected in the current Cardiac Society of Australia and New Zealand and National Heart Foundation guideline, which advocates the use of a genderless CHA2DS2-VA score.1,4
Bleeding risk: HAS-BLED score
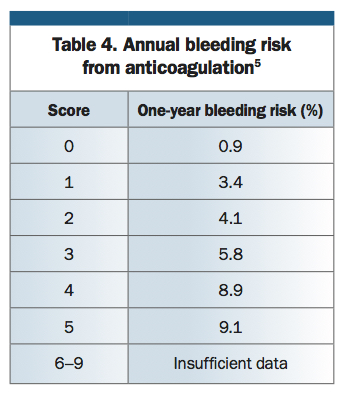
Bleeding risk assessment is far more challenging and variable. The HAS-BLED score is a commonly used risk assessment tool, traditionally applied to stratify bleeding risk in patients receiving warfarin (Table 3).5 A score of 3 or greater indicates a high one-year bleeding risk on anticoagulation, sufficient to warrant greater caution and regular clinical review (Table 4).5,6 This score does not encompass all clinically relevant factors such as known arterial venous malformations, aneurysms or history of peptic ulcer disease (with or without prior bleeding). In these cases, an individualised approach and specialist opinion may be warranted. Moreover, the HAS-BLED score has not been validated in patients receiving the new oral anticoagulants such as apixaban, rivaroxaban and dabigatran.6
{kind=link}
{kind=link}
AF and concomitant CAD
Almost 20% of patients with coronary artery disease (CAD) undergoing percutaneous coronary intervention have AF requiring long-term anticoagulation.7 Patients with an indication for long-term anticoagulation and who have concomitant CAD present a unique challenge in balancing the risks and benefits of combined anticoagulant and antiplatelet therapies (Table 2 and Table 4). Typically, this challenge arises when patients who are receiving oral anticoagulation present with an acute coronary syndrome and proceed to coronary angiography with or without percutaneous coronary intervention. Classification of antiplatelet and anticoagulant agents by mechanism and drug class is shown in the Box.
{kind=link}
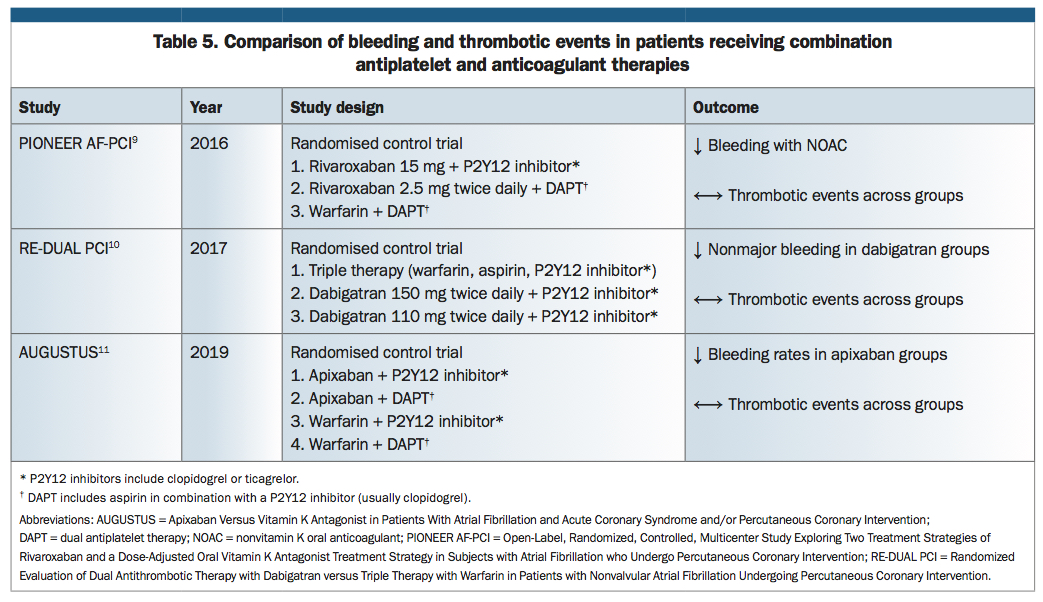
Historically, guideline recommendations in patients with dual indications (usually nonvalvular AF and an acute coronary syndrome) promoted triple therapy using warfarin and dual antiplatelet therapy (aspirin and a P2Y12 inhibitor).8 More recently, several pivotal trials, including PIONEER AF-PCI trial (Open-Label, Randomized, Controlled, Multicentre Study Exploring Two Treatment Strategies of Rivaroxaban and a Dose-Adjusted Oral Vitamin K Antagonist Treatment Strategy in Subjects with Atrial Fibrillation who Undergo Percutaneous Coronary Intervention), RE-DUAL PCI trial (Randomized Evaluation of Dual Antithrombotic Therapy with Dabigatran versus Triple Therapy with Warfarin in Patients with Nonvalvular Atrial Fibrillation Undergoing Percutaneous Coronary Intervention) and AUGUSTUS trial (Apixaban Versus Vitamin K Antagonist in Patients With Atrial Fibrillation and Acute Coronary Syndrome and/or Percutaneous Coronary Intervention), evaluated the risks and benefits of combined antithrombotic therapies (Table 5).9-11 These and other earlier clinical trials demonstrated a reduction in bleeding events with nonvitamin K oral anticoagulants (apixaban, rivaroxaban and dabigatran), and similar thrombotic events compared with warfarin therapy.12-14
{kind=link}
There is a rationale to temporarily combine an oral anticoagulant with two antiplatelet agents in patients with AF following an acute coronary syndrome with or without intervention. This is particularly relevant in the first 30 days after the event if the bleeding risk is not prohibitive, as the risk of recurrent ischaemia and stent thrombosis is highest during this period.15
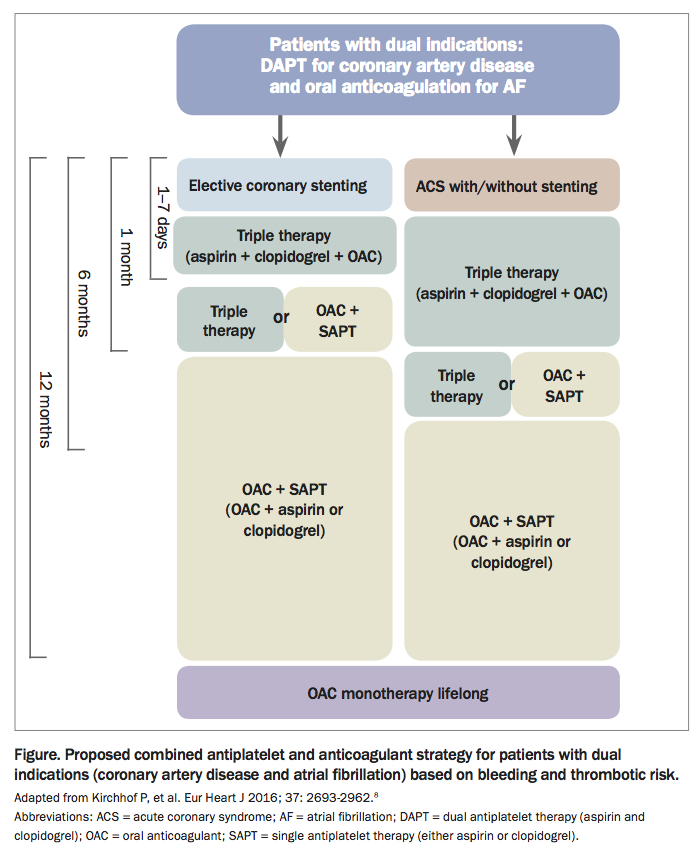
The current Australian recommendations regarding antithrombotic therapies are derived from the 2018 Cardiac Society of Australia and New Zealand guidelines (Figure).1,7,8
{kind=link}
- The duration of triple therapy (aspirin, P2Y12 inhibitor and an oral anticoagulant) should be as short as possible to mitigate bleeding risk while providing adequate antithrombotic cover during the initial high thrombotic risk period following an acute coronary syndrome and/or stenting. Triple therapy is typically prescribed for one month, followed by a single antiplatelet (usually clopidogrel) and oral anticoagulant (apixaban, rivaroxaban or dabigatran) for up to 12 months.
- In cases where dual antiplatelet therapy is required in combination with an oral anticoagulant, the recommended initial antiplatelet strategy is aspirin 100 mg daily and clopidogrel 75 mg daily.
- Clopidogrel is the preferred second antiplatelet agent over ticagrelor and prasugrel in the short term following an acute coronary syndrome or coronary stenting, as it has been more extensively studied.
- Patients with nonvalvular AF requiring long-term anticoagulation for stroke prevention who also warrant short-term dual antiplatelet therapy should be prescribed a nonvitamin K antagonist oral anticoagulants rather than warfarin in the absence of contraindications (creatinine clearance <25–30 mL/min or valvular AF).
- In cases of nonvalvular AF where an oral anticoagulant is used for stroke prevention, discontinuation of antiplatelet therapy should be considered 12 months following stent implantation or acute coronary syndrome or both, with continuation of oral anticoagulation as monotherapy.
- Proton pump inhibitors reduce gastrointestinal bleeding in high-risk patients taking aspirin, therefore the risk of gastrointestinal bleeding in patients on triple therapy may be reduced by concomitant administration of proton pump inhibitors. However, the recent changes to PBS prescribing may limit the dose and availability of this agent in the absence of an appropriate clinical indication, including gastroeosophageal reflux disease, scleroderma oesophagus or Zollinger-Ellison syndrome.
Finally, a collaborative, patient-centred approach is fundamental in establishing effective communication between healthcare providers to ensure continuity of care at the critical point of transition from the hospital environment back into the community. It is integral that communication from the in-hospital treating team to primary care providers and other relevant community stakeholders outlines clear recommendations regarding dose and duration of combined antiplatelet and anticoagulant therapies in patients with dual indications.1
Conclusion
Patient care and individual clinical circumstances tend to change over time, highlighting the importance of integrated, co-ordinated care involving appropriate specialist follow up, regular clinical review and interval risk assessment and stratification to ensure safe prescribing of antiplatelet and anticoagulation therapies. Communication between healthcare providers and patients regarding treatment objectives, care plans and changes to patient management remains vital to maintaining the fine balance between addressing cardiovascular risk while minimising bleeding sequelae. CT
References
J Am Coll Cardiol 2011; 57: 173-180.
1513-1524.