Diabetic cardiomyopathy: mechanisms, screening and treatment imperatives

Heart failure
Diabetic cardiomyopathy (DCM) refers to structural and functional changes in the heart as a consequence of diabetes that may be independent of, or in combination with, coronary disease (microvascular, macrovascular or both). As DCM tends to be asymptomatic, it is important that GPs are vigilant in screening patients early for DCM and preventing progression.
- Diabetic cardiomyopathy (DCM) has a unique pathogenesis and clinical spectrum.
- People with diabetes, especially women, have an increased risk of heart failure (HF), independent of traditional cardiac risk factors.
- The initial cellular and structural changes in DCM, such as cardiac fibrosis, usually precede the onset of symptoms.
- Initially, there may only be left ventricular hypertrophy before onset of left ventricular diastolic dysfunction and, finally, overt systolic dysfunction.
- People with diabetes and HF have a higher mortality rate. Overt systolic dysfunction confers a poor prognosis.
- High-risk patients should be identified and screened with ECG and echocardiography.
- Detecting changes in strain parameters on echocardiography is pivotal in making a prompt diagnosis and early referral to a cardiologist.
- Cardiac MRI is emerging as a useful and sensitive tool for early identification of structural changes associated with DCM, including signs that cannot be identified on an echocardiogram; however, access in the community is limited.
- Aggressive treatment of modifiable cardiac risk factors is imperative to prevent progression of HF.
- Good glycaemic control is important; however, intensive control (glycated haemoglobin level below 6%) is not beneficial and may cause harm.
- Treatment with SGLT-2 inhibitors is showing promise in targeting the metabolic changes and reduces HF hospitalisations in people with diabetes, beyond the effect on blood glucose levels.
- An integrated approach involving a heart failure care team, diabetic educator and cardiologist is pivotal.
Diabetes mellitus is associated with an array of well-known microvascular and macrovascular complications, with atherosclerotic cardiovascular disease (CVD) being the leading cause of mortality in patients with diabetes.1 The incidence and prevalence of heart failure (HF) is increased in individuals with diabetes, and clinical outcomes are worse in these patients.2 Although HF may arise from macrovascular coronary artery disease, the most common causes are nonischaemic.3 Diabetic cardiomyopathy (DCM) describes the presence of abnormal myocardial structure and function in the absence of other cardiac disease risk factors (obstructive coronary artery disease, hypertension, dyslipidaemia). This definition, however, dates back to the 1970s and may not be as useful today, given the common overlap of these comorbidities.
Fibrosis, left ventricular hypertrophy (LVH) and abnormal cellular signalling characterise DCM. Progression of these initial abnormalities leads to sequential development of subclinical diastolic dysfunction, HF with preserved ejection fraction (HFpEF) and, finally, reduced ejection fraction.2 The structural and functional changes in the myocardium of people with diabetes is unique and we are beginning to understand the underlying cellular changes that lead to the ultimate pathological changes in the myocardium. DCM is common, although it is frequently underdiagnosed because most patients with DCM are asymptomatic and there is no clear screening algorithm.
A further challenge in the identification of DCM is the current definition, which suggests that DCM occurs in isolation of other cardiovascular (CV) risk factors. Comorbidities, including hypertension and hypercholesterolaemia, are common in people with diabetes. The presence of these additional cardiac risk factors can lead to additional non-DCM related myocardial damage. In particular, diabetic patients with comorbidities, including obesity and obstructive sleep apnoea, are at increased risk of developing myocardial hypertrophy independent of DCM; however, all of these patients warrant investigation and intervention when appropriate.
The link between heart failure and diabetes
The prevalence of HF in Australia is 1.0 to 2.0% and increases significantly with age. The principal risk factors for HF are coronary artery disease, diabetes and hypertension. Despite significant expenditure on public health prevention strategies and effectively subsidised medical therapies, the burden of both HF and diabetes in Australia continues to rise.4 However, there is very little evidence available on the prevalence of DCM and patient outcomes.5
The relationship between HF and diabetes has been well demonstrated. The Framingham Study reported a twofold increased risk of HF in men with diabetes and a fivefold increased risk in women with diabetes. This elevated risk is independent of traditional cardiac risk factors, including coronary artery disease, cholesterol levels, weight, blood pressure and age.6 In hospitalised patients with a new diagnosis of HF, more than half were found to have impaired glucose tolerance or DM.7-9
Not only is there a clear link between diabetes and HF, outcomes for patients with HF who have diabetes are worse.2 There is 1.5-fold increase in one-year mortality from HF for people with diabetes compared with those without.3 Similarly, there are increased rates of hospital admission for HF among people with diabetes, including those without systolic dysfunction.10
The increased prevalence of HF in people with diabetes is not exclusive to those with type 2 diabetes. In a prospective study of people with asymptomatic type 1 diabetes in Melbourne, 29% of the cohort had abnormal echocardiograms. In those with abnormal echocardiograms, 69% had diastolic dysfunction and 10% had systolic dysfunction. The group with systolic dysfunction were older than those with diastolic dysfunction and serial echocardiography demonstrated worsening dysfunction over time, which is supportive of DCM being a progressive pathology.11
Risk factors
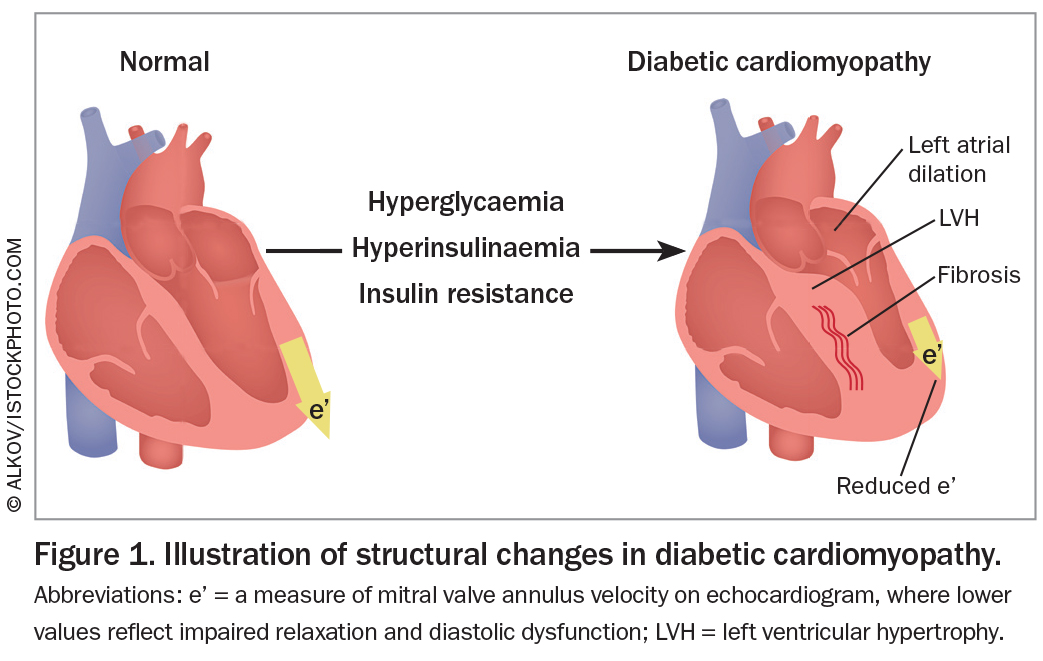
The development of DCM is principally linked to blood glucose control. Hyperglycaemia, systemic insulin resistance and hyperinsulinaemia are the clinical abnormalities in diabetes and are all involved in the pathogenesis and progression of DCM.2,12 Each 1% increase in glycated haemoglobin (HbA1c) level is associated with an 8 to 15% increased risk of HF.12,13 There is similarly a linear relationship between increasing HbA1c and admissions to hospital with HF.13 There is strong evidence that prediabetic insulin-resistant states, including obesity, are also linked to the development of myocardial changes independent of other CV risk factors. There is a 17% increased risk of an abnormal echocardiogram with each unit increase in body mass index.11
Pathophysiology
Structural changes
The Strong Heart Study demonstrated clear differences in the myocardium of people with diabetes.14 There is increased left ventricular (LV) wall thickness and mass (most marked in women with diabetes) independent of arterial blood pressure. LVH and fibrosis result in a reduction in LV cavity size and impaired myocardial relaxation (Figure 1). Most patients remain asymptomatic until there is eventual systolic dysfunction (Figure 2).
{kind=link}
{kind=link}
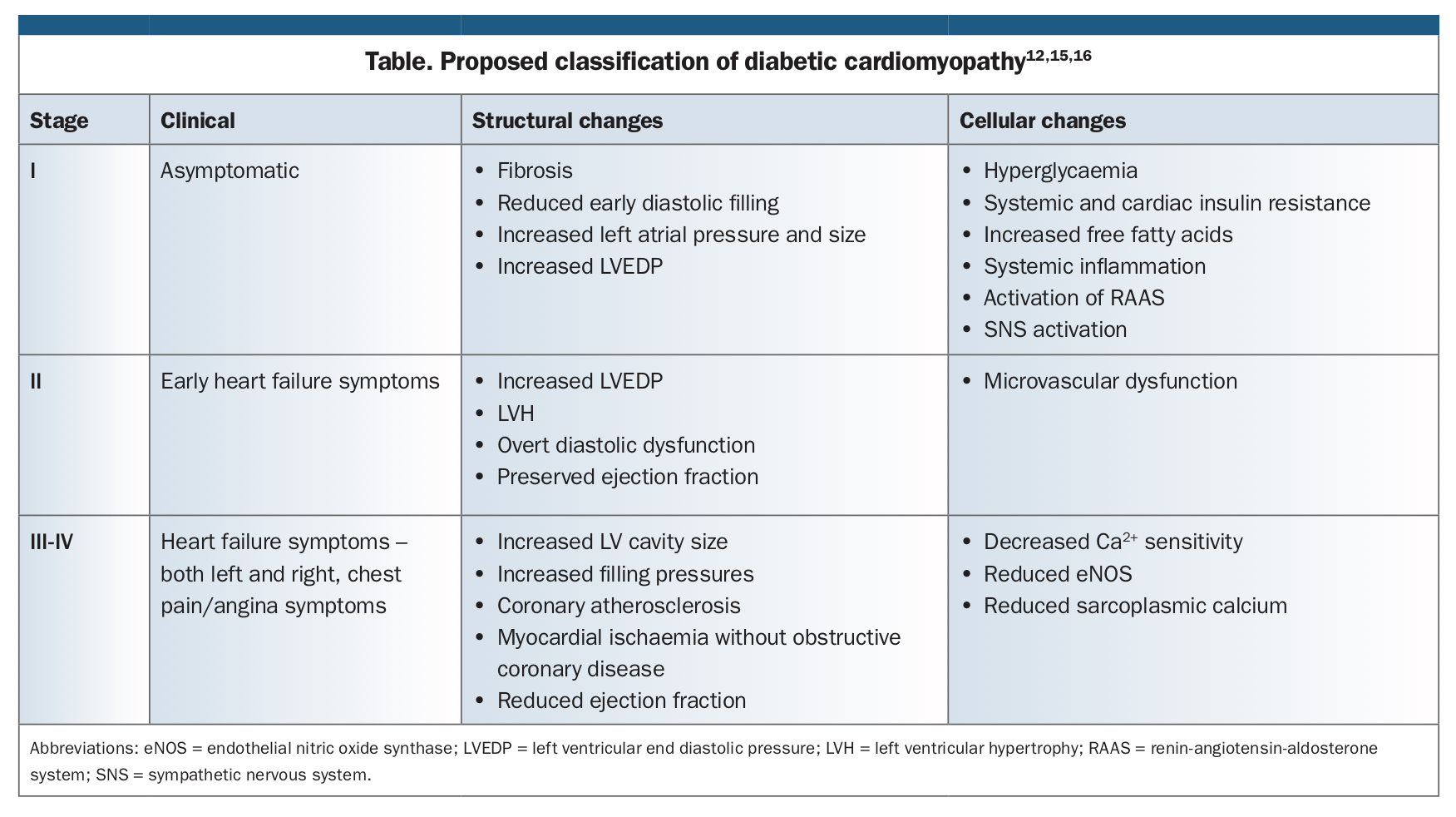
The early diastolic changes are probably under-reported using traditional echocardiographic parameters, which is a dynamic field in itself. The proposed classification for the stages of DCM reflects the clinical and pathological spectrum of the disease. This classification is summarised in the Table.12,15,16
{kind=link}
Cellular changes
The effects of hyperglycaemia and systemic and myocardial insulin resistance are vast, complex and not completely understood. Changes in fatty acid metabolism result in myocardial reliance on fatty acid beta oxidation.12 The effect of insulin resistance and reductions in insulin lead to the production of reactive oxygen species and impaired calcium homeostasis in the myocardium, which results in myocardial fibrosis and a reduction in effective contractility. Additionally, the production of advanced glycation end products causes activation of proinflammatory cascades, contributing to cardiac fibrosis and a reduction in myocardial compliance.
There is emerging evidence that cardiac autonomic neuropathy is associated with LV systolic dysfunction due to the dominance of sympathetic tone.12,17 This results in persistent release of catecholamines in the myocardium and further exacerbates the myocardial remodelling process.
Screening for DCM
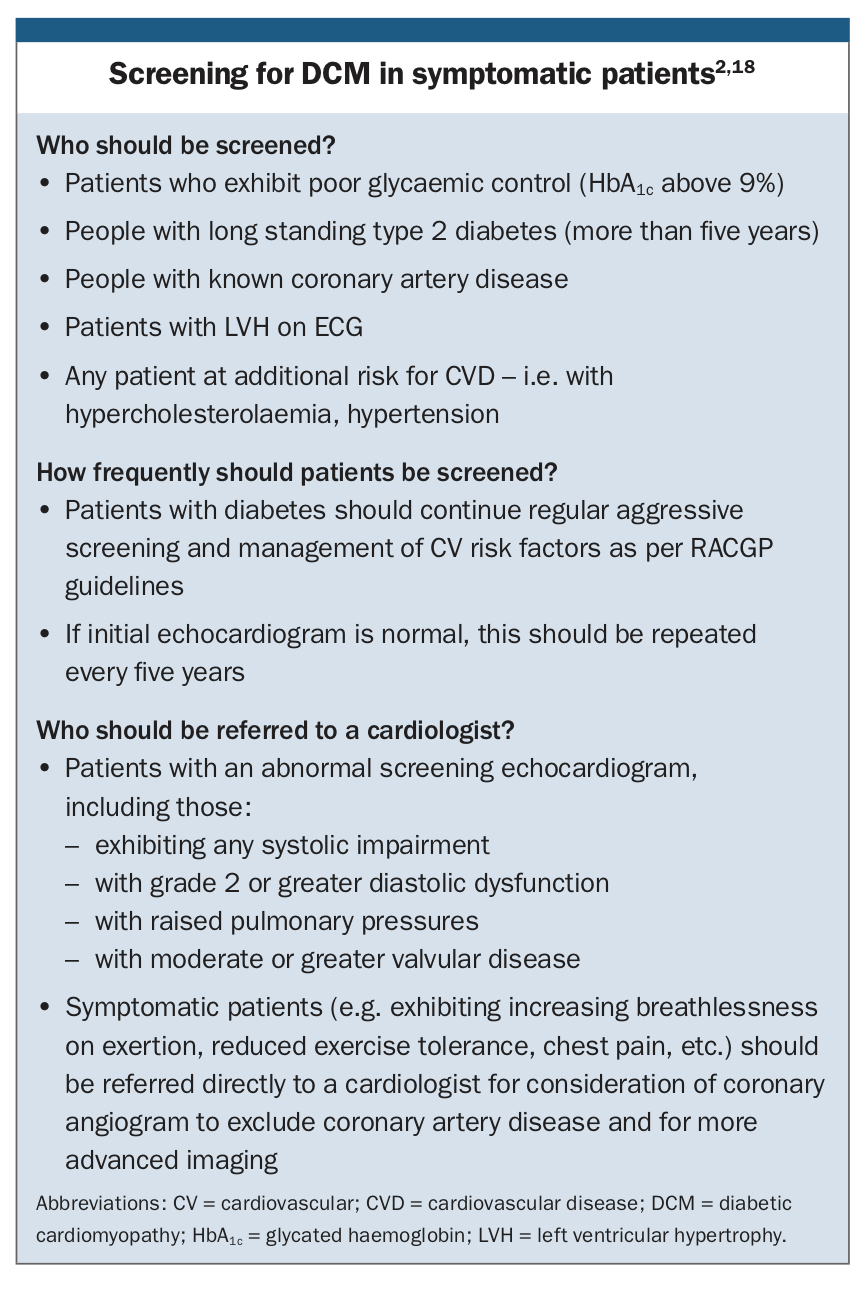
The key challenge for clinicians, and in particular GPs, is that patients in the early spectrum of DCM are generally asymptomatic, whereas symptomatic HF (reduced exercise tolerance, dyspnoea, oedema, etc.) is unlikely to be missed by GPs. The progressive nature of DCM and poor outcomes in advanced disease mean that early detection of DCM and prevention of progression is paramount. In patients who are symptomatic, it is important to assess for obstructive coronary artery disease (given the burden of ischaemic heart disease among people with diabetes) and to consider advanced imaging techniques to assess for DCM – hence, we recommend that these (i.e. symptomatic) patients should be referred to a cardiologist. Screening for DCM in symptomatic patients is summarised in the Box.12,18 The Flowchart outlines our suggested screening pathway for asymptomatic patients.18
{kind=link}
Methods of screening
Focused screening should include investigating traditional cardiac risk factors. Advanced imaging techniques, such as cardiac MRI and echocardiography with strain and doppler parameters, are useful in these early stages, although can be difficult to access in the community, are costly and require skilful interpretation.12,17 Cardiac biomarkers are of limited usefulness in screening for HF.
Echocardiography
Echocardiography is a reliable and relatively inexpensive tool for evaluating DCM. Echocardiography is useful in defining systolic dysfunction, and when interpreted accurately, changes in strain and doppler parameters may be diagnostic for DCM in the subclinical phase. Strain echocardiography is a noninvasive measure of myocardial deformation in multiple directions (longitudinal, radial, circumferential) and provides a more accurate assessment of contractile function.19
More than 25% of people with diabetes have abnormalities in systolic strain preceding onset of diastolic dysfunction.12 As the LV cavity becomes smaller and less compliant, diastolic dysfunction, as demonstrated by changes in tissue-Doppler parameters, ensues. Late diastolic dysfunction is seen in atrial dilatation and rapid early diastolic filling.12 These changes eventually manifest as a global impairment in contractility and reduction in ejection fraction. Therefore, in the hands of a skilled sonographer and clinician, DCM may be detected early.
ECG
In the absence of overt cardiac failure or ischaemia, subtle changes may be observed in the electrocardiogram of a patient with DCM, which may represent early cardiac fibrosis, LVH or diastolic dysfunction.20 The preclinical phase of DCM may be diagnosed by demonstrating exercise-induced LV dysfunction or resting LVH.20 The EURODIAB Insulin-Dependent Diabetes Mellitus Complications Study investigated 3250 people with long standing type 1 diabetes and found the prevalence of LVH was three times that of the age-matched general population.21
Biomarkers
The use of cardiac biomarkers for early detection of DCM remains controversial. The most widely established and validated are B-type natriuretic peptide (BNP) and the N-terminal fragment of its prohormone (NT-proBNP). These hormones are released in the setting of increased fluid volume, manifesting as ventricular stretch and cardiac remodelling.22
These biomarkers are useful for supporting a diagnosis of HF in undifferentiated or multifactorial dyspnoea. However, their utility in detecting mild systolic dysfunction or diastolic dysfunction is limited.5 In an Australian population-based cohort, BNP and NT-proBNP were poor markers of mild systolic and diastolic dysfunction; however, they were increased in patients with moderate to severe systolic dysfunction.23 The accuracy of these biomarkers may be confounded in patients with hypertension, diabetes, coronary artery disease, renal impairment, obesity and older age.3,22,23
Other biomarkers such as high sensitivity C-reactive protein and troponins T, N and I have also been investigated and, although they may be elevated in patients with diabetes and HF, no clear correlation with DCM has been shown.17
Cardiac MRI
Cardiac MRI is rapidly evolving as the means of diagnosing all types of cardiomyopathy, and in particular, the subclinical phase of DCM. It may demonstrate myocardial fibrosis and early markers of diastolic dysfunction, which when coupled with novel mapping techniques to characterise the extracellular matrix (i.e. how stiff or fibrosed the myocardium has become) is expected to soon allow characterisation of different HFpEF phenotypes. However, lack of access to and the high cost of cardiac MRI and cardiac positron emission tomography scans limits their use. There are currently no Medicare rebatable indications for these imaging studies for DCM or HFpEF.
Treatment strategies
Treatment of symptomatic HF in people with diabetes is guideline-directed, as for all patients with HF. 24 Management of traditional CV risk factors is imperative as comorbidities such as hypertension and coronary artery disease may worsen diastolic and systolic HF. These risk factors should be addressed and managed according to the guidelines.24,25
Treatment of hyperglycaemia and insulin resistance to prevent and avoid precipitating HF is more complicated. Sodium-glucose cotransporter-2 (SGLT-2) inhibitors have received increased attention owing to their benefit in preventing HF admissions, independent of glycaemic control.9 Conversely, some medications such as thiazolidinediones are known to worsen HF.
Lifestyle measures
As for all people with diabetes, attention to modifiable risk factors prevents and improves important end organ complications, especially CVD. They are cheap interventions and improve quality of life. An excessively sedentary lifestyle, obesity and poor diet contribute to insulin resistance. There are observed reductions in HF events with weight loss and exercise.3,26
Multimodal approach
Involvement of diabetic educators and HF nurses is imperative in the short- and long-term management of DCM. HF nurses play a pivotal role in patient education, early detection of exacerbations and prevention of frequent HF hospitalisations.
Pharmacological management
Until recently, no large randomised control trials have had HF prevention as a primary end point. As mentioned earlier, there is evidence to suggest a linear relationship between HbA1c level and risk of HF. Intensive glycaemic control has not demonstrated a reduction in HF hospital admissions, mortality or macrovascular events, including CV events.27-29 There is also evidence of increased mortality when targeting an HbA1c of below 6%.28
Recently, a randomised control trial showed clear and consistent benefits with an oral antidiabetic agent (dapagliflozin) in preventing HF hospitalisations and other key CV outcomes in people with type 2 diabetes and those with no diabetes.8 Importantly, there was a significant benefit observed beyond the effect on HbA1c and diabetic status. There is also increasing evidence of benefits from metformin and glucagon-like peptide 1 (GLP-1) agonists to people with diabetes at risk of HF, independent of their effect on blood glucose levels.
Metformin
Metformin is the most widely used agent for controlling blood glucose levels, given its safety profile and relatively low cost. The evidence for the use of metformin in HF has been confusing, as it was thought to increase mortality owing to the risk of lactic acidosis, although this has not been seen in large-scale observational studies.29,30 Its use may also be difficult or contraindicated in patients with HF who have coexisting renal dysfunction or cardiorenal syndrome. A series of observational studies have demonstrated that those with HF who were taking metformin had lower morbidity and mortality compared with control groups.30,31 The mechanism for this is yet to be completely understood.
SGLT-2 inhibitors
Sodium-glucose cotransporters (SGLTs) are proteins expressed in the proximal tubule of the nephron involved in glucose homeostasis. The SGLT-2 inhibitors promote glycosuria and reduce reabsorption of glucose back into circulation. The glucose-lowering effect is independent of insulin and the ability to lower glucose is limited by the filtered glucose and osmotic diuresis. The glycosuria and diuresis have multiple metabolic effects including weight loss, improved blood pressure and reduced albuminuria.
This class of medication has received recent attention due to its unique benefit in CVD (specifically HF) and renal disease in people with and without diabetes. A number of large randomised control trials have shown reduced CV events, HF hospitalisations and CV deaths, as well as reduced renal progression with SGLT-2 inhibitor use.9,32 Most SGLT-2 inhibitors have a good safety profile and are well tolerated as oral tablets.
The DAPA-HF trial showed the primary composite outcome of worsening HF or CV death was 26% lower in patients receiving dapagliflozin compared with placebo, independent of diabetic status. There was reduced all-cause mortality and improved HF symptoms. The marked benefit independent of an improvement in HbA1c level suggests that there are additional metabolic and cellular mechanisms beyond glucosuria. The effects on weight, blood pressure, haematocrit, renal function and NT-proBNP were also similar in those with and without diabetes.8
In Australia, SGLT-2 inhibitors are not yet PBS subsidised for treating DCM or as monotherapy for people with diabetes. Currently, they can be used as combination therapy, or when first-line treatment is contraindicated, and when the HbA1c level is above 7%.
Although the metabolic and cellular effects of SGLT-2 inhibitors are showing promise in mitigating risk of HF in people with diabetes, there is still no definitive evidence of a benefit in diastolic dysfunction or in the prevention of DCM.
GLP-1 agonists/DPP-4 inhibition
Incretins, such as GLP-1 agonists, are peptides that increase insulin in a glucose-dependent manner. They regulate postprandial glucagon secretion, slow gastric emptying and increase satiety.33 GLP-1 agonists have shown promise, with improvements in weight, blood pressure and lipid profile in people with type-2 diabetes.34 Although their use in mitigating CV risk factors is established and encouraged, owing to a good safety profile, there have been no large-scale randomised controlled trials that have shown a benefit in preventing or improving HF, and preclinical trials have demonstrated no definitive risk of worsening HF.35,36
Dipeptidyl peptidase-4 (DPP-4) inhibitors are know to inactivate GLP-1 activity and have become popular in helping to control hyperglycaemia in people with type-2 diabetes, owing to the option of an oral daily tablet. Their role in preventing diabetic cardiomyopathy has not been studied in large-scale human trials; however, there are promising benefits in modulating CV risk.37 There are fewer side effects, they can be prescribed to patients with moderate renal dysfunction and there is less weight gain compared with other antidiabetic agents. Saxagliptin, however, has been documented to increase CV risk in patients with myocardial ischaemia (MI) and is not recommended for such patients.38,39
Sulfonylureas
The evidence for the use of sulfonylureas has been confusing in people with HF and MI. It has been postulated that they prevent the protective ischaemic preconditioning that is the adaptive response following MI.33 A large meta-analysis of randomised controlled trials did not show an association between sulfonylureas and increased risk of all-cause death, CV death, MI or stroke.40
Sulfonylureas have been associated with an increased trend towards HF when used as monotherapy compared with metformin monotherapy, and the risk increased with increased dose.39,41 Gliclazide has been suggested to be the safest of this class of drugs. The trend towards harm from sulfonylureas may be linked to weight gain, hypertension, hypoglycaemia or ischaemic preconditioning.42 There is no definite evidence that sulfonylureas worsen HF but, to date, there is no convincing evidence that they play a role in the prevention of DCM.
Thiazolidinediones
Thiazolidinedione use in people with diabetes with CVD is controversial. There is well-documented evidence that their use as monotherapy or in combination causes weight gain and fluid retention.42 Studies have consistently shown increased HF hospitalisations in patients on pioglitazone.42-44 The perceived benefit of pioglitazone may be due to its effects on reducing circulating triglycerides and free fatty acids, thereby increasing HDL cholesterol.44 It has also been shown to reduce microalbuminuria.43 However, pioglitazone does not prevent DCM and is not recommended for patients at risk of HF or those with symptomatic HF (NYHA Class II and above), and should be promptly discontinued if there are any signs suggestive of HF.
Novel agents
Some preclinical studies are exploring alternative agents for reducing oxidative stress and myocardial fibrosis in patients with DCM. In a study using rat models, atorvastatin reduced myocardial fibrosis and inflammation and improved LV function independently of the LDL-cholesterol-lowering capacity.45 Coenzyme Q10 supplementation as an adjunct in chronic HF was shown to be safe and effective at reducing major adverse CV events, but this is not specific to DCM.
In an experimental model of DCM, fenofibrate had a mild benefit in reducing myocardial damage when studied alongside metformin, demonstrating a reduction in total fat accumulation, but not myocardial fibrosis.46 Other experimental studies that have shown promise in the prevention of DCM include the ACE inhibitor captopril, nebivolol, spironolactone and zinc supplementation.47 These agents are not yet indicated for prevention of DCM and more research is needed.
Conclusion
DCM is underdiagnosed and places a significant burden on healthcare systems in Australia. Given that patients with DCM have worse outcomes than those without diabetes with HF, there is a need for screening algorithms and integrated care models. These patients have complex comorbidities and the role of the GP is essential to aid in early detection, prompt and appropriate referral, and to address gaps in patient education. CT